


RINVOQ vs
HUMIRA® (adalimumab)
SELECT-SWITCH Study in RA
Explore head-to-head data for RINVOQ vs HUMIRA in moderate to severe rheumatoid arthritis patients who have had an inadequate response or intolerance to 1 TNFi.
US-MULT-250253
WARNING: Serious Infections, Mortality, Malignancies, Major Adverse Cardiovascular Events, and Thrombosis
RINVOQ achieved DAS28-CRP <2.6* and DAS28-CRP ≤3.2 (ranked secondary endpoints) at Week 12 or 14, with durable remission and low disease activity rates out to ~5 years.1-6
*Does not mean drug-free remission or complete absence of disease activity.
INDICATION
RINVOQ is indicated for the treatment of adults with moderately to severely active rheumatoid arthritis (RA) who have had an inadequate response or intolerance to one or more tumor necrosis factor (TNF) blockers.
Limitations of Use: RINVOQ is not recommended for use in combination with other Janus kinase (JAK) inhibitors, biologic disease-modifying antirheumatic drugs (bDMARDs), or with potent immunosuppressants such as azathioprine and cyclosporine.
NRI Data From SELECT-BEYOND (bDMARD-IR)1,7
RINVOQ 15 mg + csDMARD (n=164), placebo + csDMARD (n=169)
ACR20 | PRIMARY ENDPOINT
65%* RINVOQ vs 28% placebo at Week 12
*P<0.0001 RINVOQ vs placebo.
SELECT-BEYOND (Study RA-V)1,7:
24‑week, randomized, double-blind, placebo-controlled study of 499 adult patients with moderate to severe RA who had an inadequate response or intolerance to bDMARDs. Patients on background csDMARDs were randomized to receive RINVOQ 15 mg once daily (n=164) or placebo (n=169). The primary endpoint was ACR20 response at Week 12.
NRI Data From SELECT-MONOTHERAPY (MTX-IR)1,2
RINVOQ 15 mg (n=217), cMTX (n=216)
ACR20 | PRIMARY ENDPOINT
68%* RINVOQ vs 41% MTX at Week 14
*P<0.0001 RINVOQ vs MTX.
RINVOQ IS INDICATED FOR TNFi-IR PATIENTS.
SELECT-MONOTHERAPY (Study RA-II)1,2:
14‑week, randomized, double‑blind, active comparator‑controlled study of 648 adult patients with moderate to severe RA who had an inadequate response to MTX. The primary endpoint was ACR20 response at Week 14.
bDMARD=biologic disease-modifying antirheumatic drug; CRP=C-reactive protein; DAS28-CRP=28 joint disease activity score using C-reactive protein; DMARD=disease-modifying antirheumatic drug; IR=intolerance or inadequate response; JAK=Janus kinase; LDA=low disease activity; MTX=methotrexate; TNF=tumor necrosis factor; TNFi=tumor necrosis factor inhibitor.
Please see Important Safety Information, including BOXED WARNING on Serious Infections, Mortality, Malignancies, Major Adverse Cardiovascular Events, and Thrombosis, below.
REMISSION:
(DAS28-CRP <2.6*)
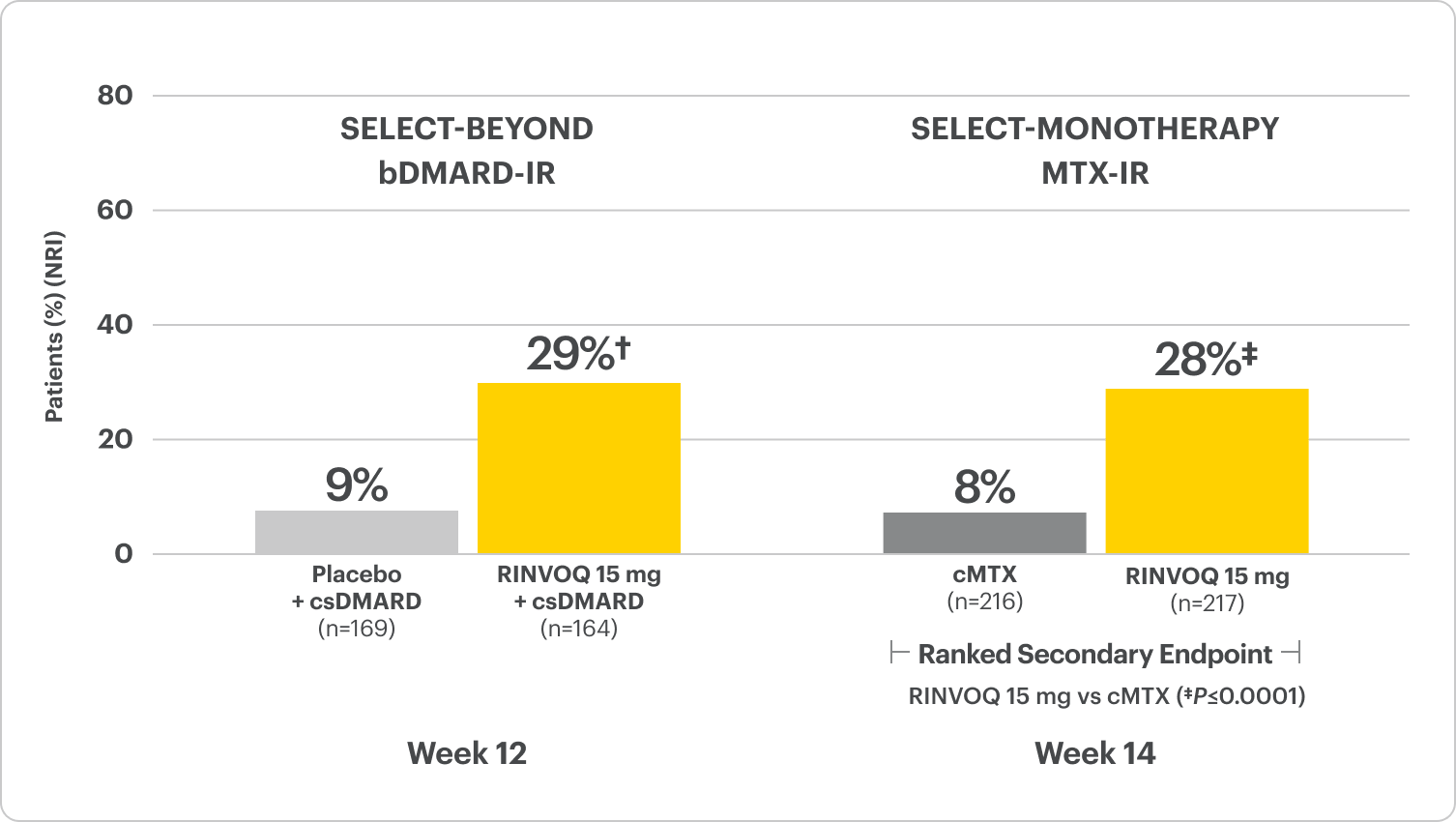
RINVOQ is indicated for TNFi-IR patients.
†P≤0.001 for RINVOQ + csDMARDs vs placebo + csDMARDs; analysis was not controlled for multiplicity. P-value obtained through nominal statistical testing.
*Clinical remission does not mean drug‑free remission or complete absence of disease activity.
DATA LIMITATIONS:
Data not labeled as a ranked secondary endpoint were prespecified nonranked endpoints not controlled for multiplicity; therefore, treatment differences could represent chance findings. No conclusions regarding these comparisons can be made.
LDA:
(DAS28-CRP ≤3.2)
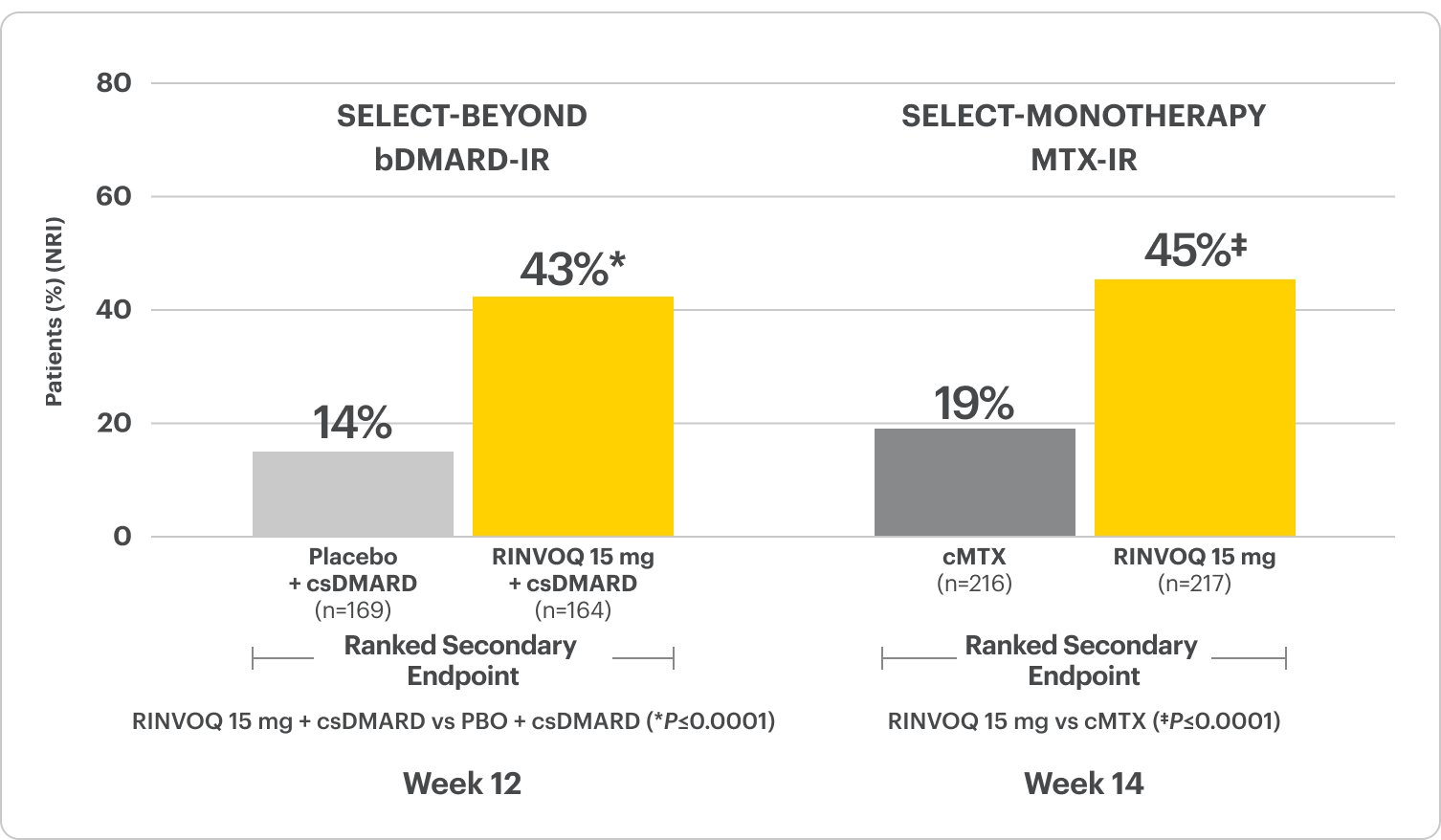
RINVOQ is indicated for TNFi-IR patients.
SELECT-BEYOND:
bDMARD-IR Patients
ALL DATA AS OBSERVED (AO)
DAS28-CRP <2.6*
66% of RINVOQ + csDMARDs patients achieved clinical remission at Week 260
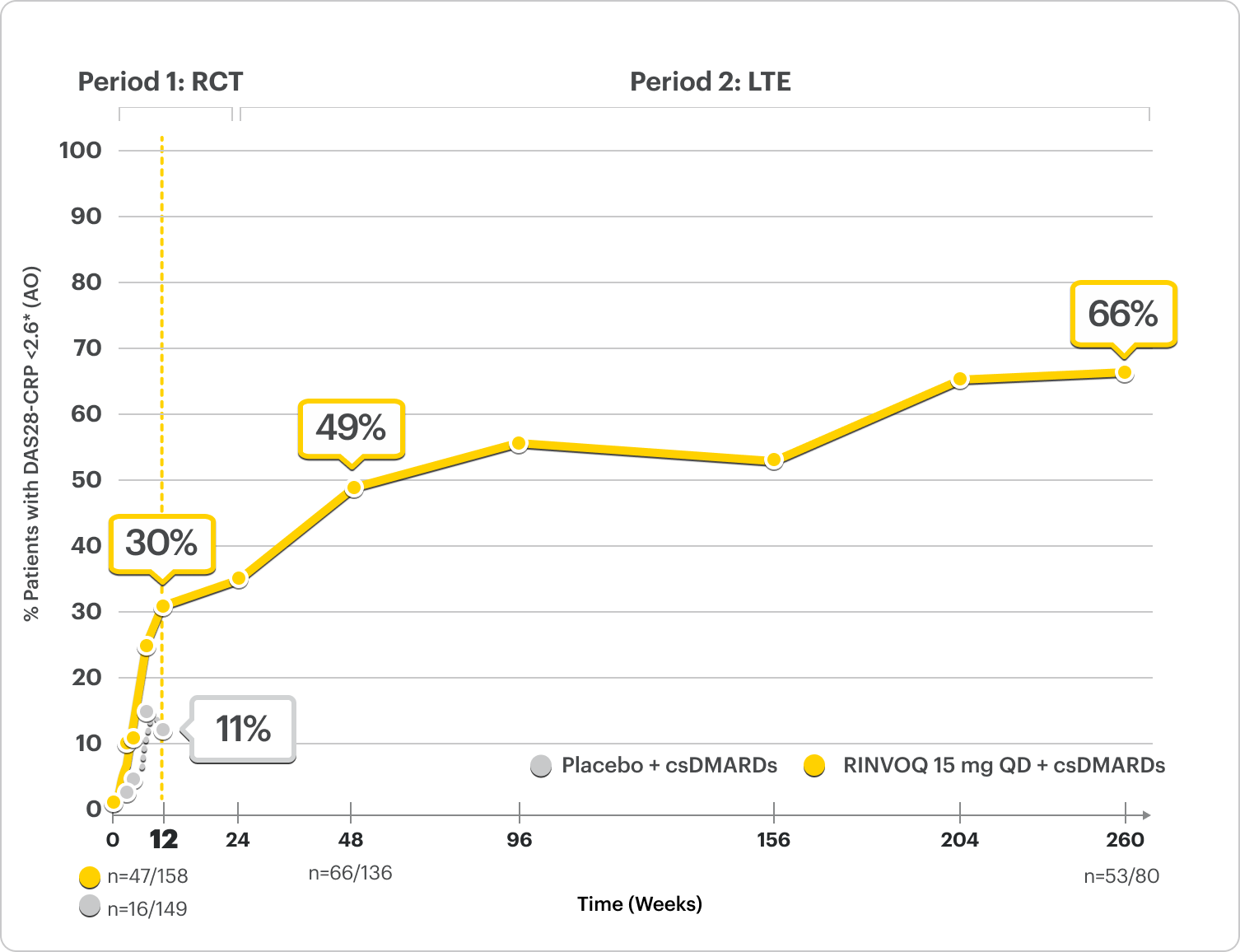
RINVOQ is indicated for TNFi-IR patients.
Starting at Week 24, initiation of or change in corticosteroids, NSAIDs, acetaminophen, and csDMARDs was permitted. Patients not achieving response criteria ≥20% improvement in SJC and TJC at two consecutive visits were removed from the study.
*Clinical remission does not mean drug-free remission or complete absence of disease activity.
SELECT-MONOTHERAPY:
MTX-IR Patients
ALL DATA AS OBSERVED (AO)
DAS28-CRP <2.6*
71% of RINVOQ patients achieved clinical remission at Week 260
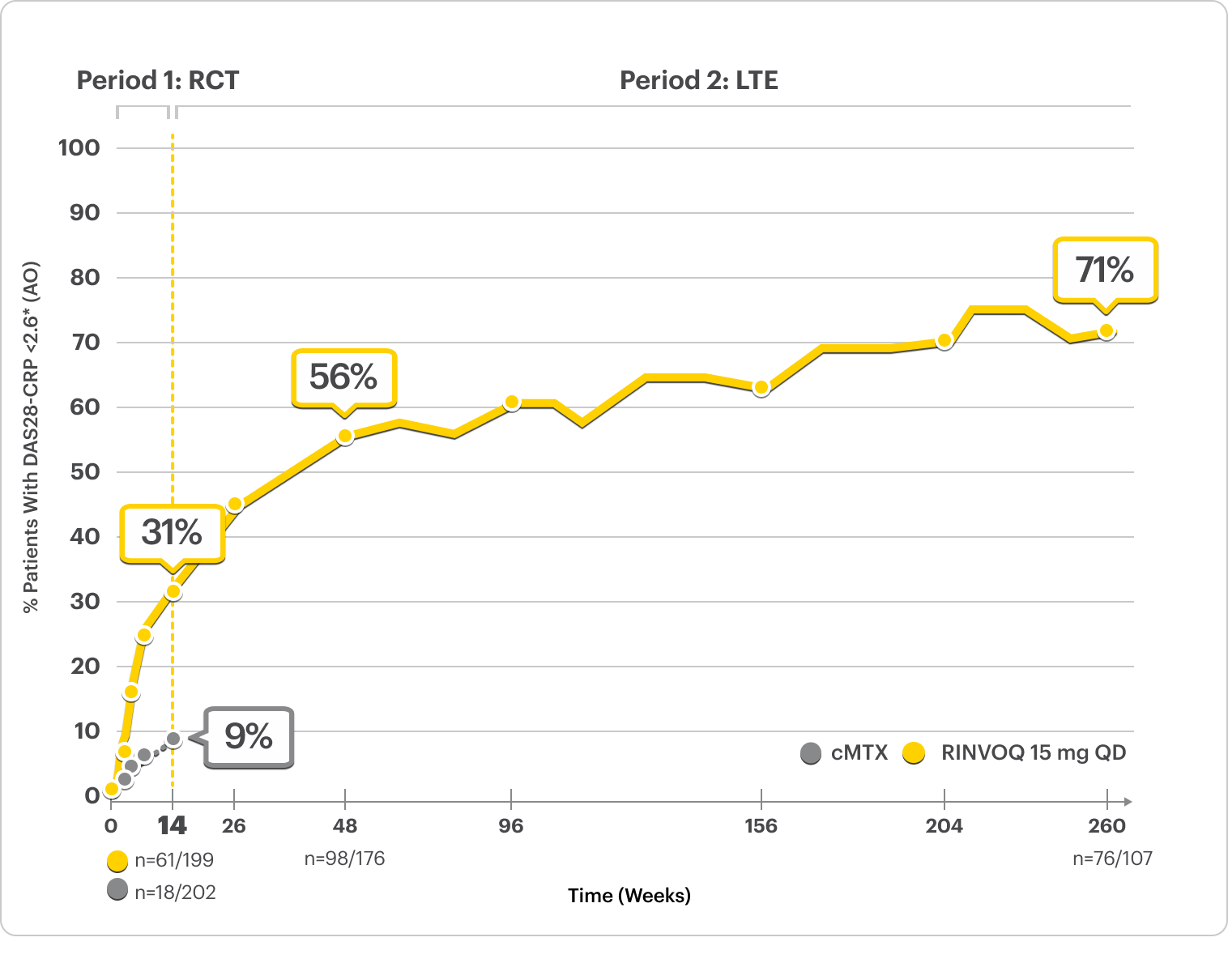
RINVOQ is indicated for TNFi-IR patients.
Treatment groups were by initial randomization. Starting at Week 26, initiation of or change in corticosteroids, NSAIDs, acetaminophen or ≤2 csDMARD was allowed for patients who did not achieve CDAI ≤10.
*Clinical remission does not mean drug-free remission or complete absence of disease activity.
In an As Observed (AO) analysis, patients with missing data at a specific time are not included, which may enrich the population and increase the response rates.
LTE LIMITATIONS: There is potential for enrichment of LTE data; unblinding patients may cause bias related to overall treatment effect.
Serious Infections: RINVOQ-treated patients are at increased risk of serious bacterial (including tuberculosis [TB]), fungal, viral, and opportunistic infections leading to hospitalization or death. Most patients who developed these infections were taking concomitant immunosuppressants, such as methotrexate or corticosteroids.
Mortality: A higher rate of all-cause mortality, including sudden cardiovascular (CV) death, was observed with a Janus kinase inhibitor (JAKi) in a study comparing another JAKi with tumor necrosis factor (TNF) blockers in rheumatoid arthritis (RA) patients ≥50 years with ≥1 CV risk factor.
Malignancies: Malignancies have occurred in RINVOQ-treated patients. A higher rate of lymphomas and lung cancer (in current or past smokers) was observed with another JAKi when compared with TNF blockers in RA patients.
Major Adverse Cardiovascular Events: A higher rate of CV death, myocardial infarction, and stroke was observed with a JAKi in a study comparing another JAKi with TNF blockers in RA patients ≥50 years with ≥1 CV risk factor. History of smoking increases risk.
Thromboses: Deep venous thrombosis, pulmonary embolism, and arterial thrombosis have occurred in patients treated for inflammatory conditions with JAK inhibitors, including RINVOQ. A higher rate of thrombosis was observed with another JAKi when compared with TNF blockers in RA patients.
Hypersensitivity: RINVOQ is contraindicated in patients with hypersensitivity to RINVOQ or its excipients.
Other Serious Adverse Reactions: Hypersensitivity Reactions, Gastrointestinal Perforations, Laboratory Abnormalities, and Embryo-Fetal Toxicity.
SELECT-BEYOND:
bDMARD-IR Patients
ALL DATA AS OBSERVED (AO)
LDA (DAS28-CRP ≤3.2)
81% of RINVOQ + csDMARDs patients achieved LDA at Week 260
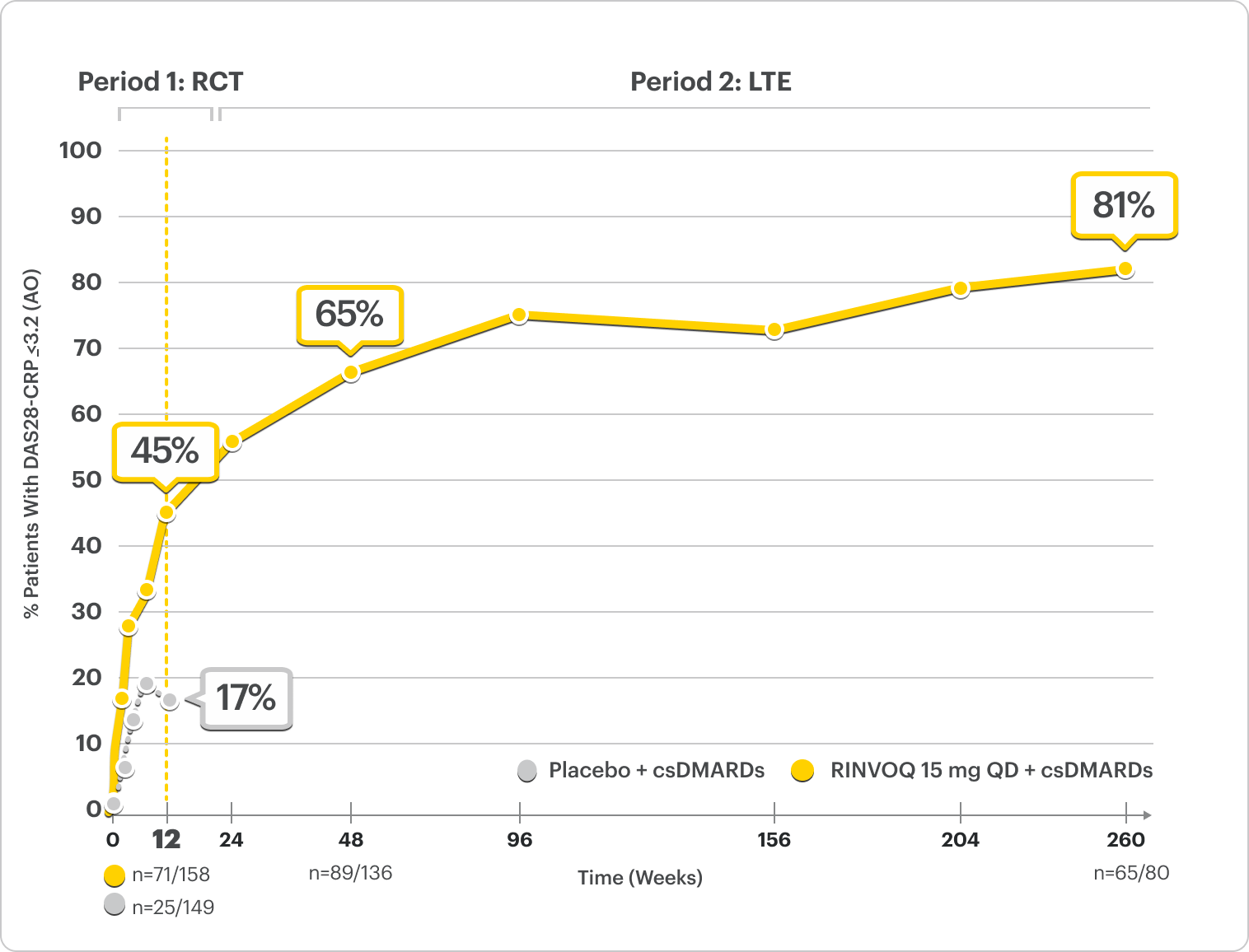
RINVOQ is indicated for TNFi-IR patients.
Starting at Week 24, initiation of or change in corticosteroids, NSAIDs, acetaminophen, and csDMARDs was permitted. Patients not achieving response criteria ≥20% improvement in SJC and TJC at two consecutive visits were removed from the study.
SELECT-MONOTHERAPY:
MTX-IR Patients
ALL DATA AS OBSERVED (AO)
LDA (DAS28-CRP ≤3.2)
89% of RINVOQ patients achieved LDA at Week 260
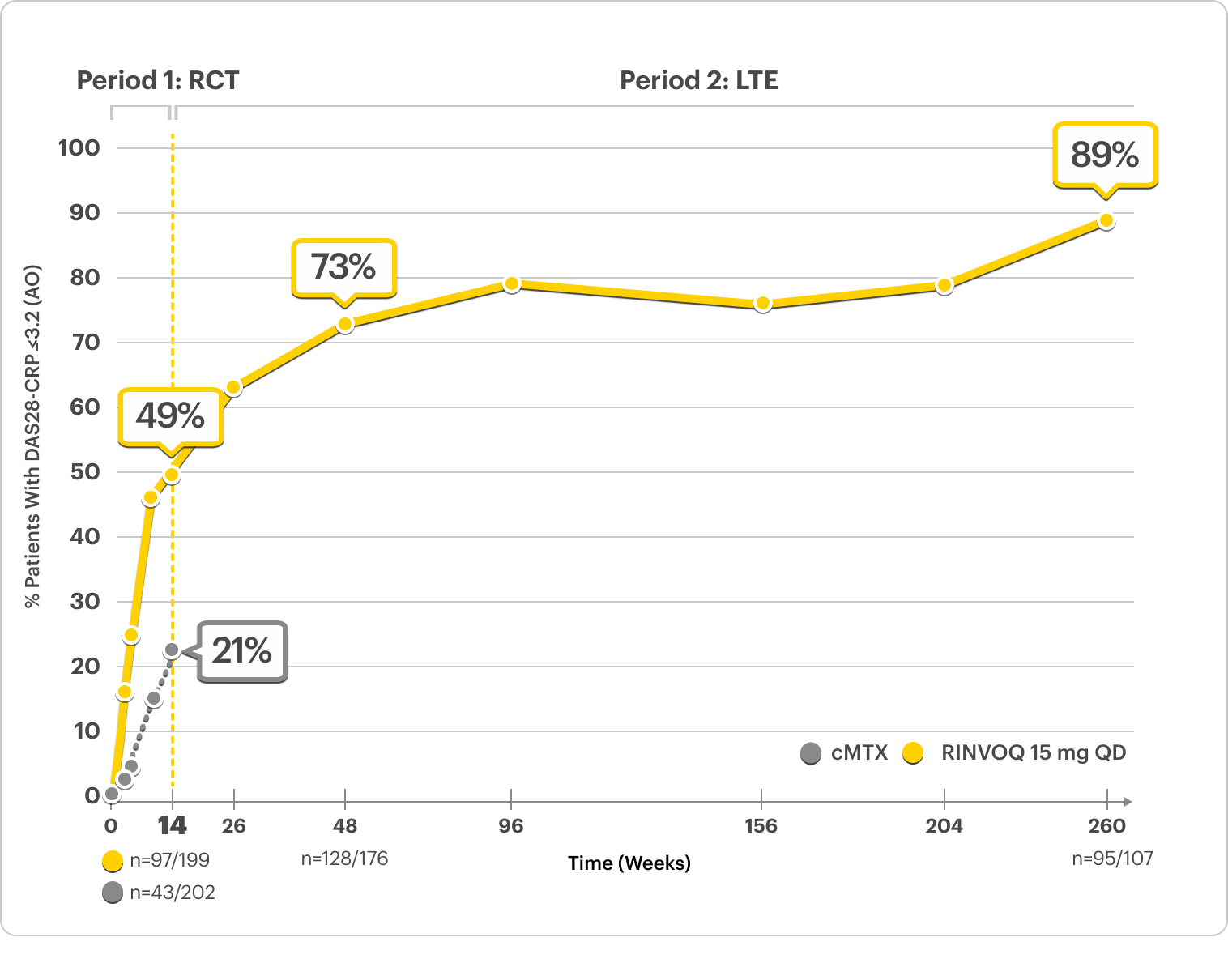
RINVOQ is indicated for TNFi-IR patients.
Treatment groups were by initial randomization. Starting at Week 26, initiation of or change in corticosteroids, NSAIDs, acetaminophen or ≤2 csDMARD was allowed for patients who did not achieve CDAI ≤10.10
In an As Observed (AO) analysis, patients with missing data at a specific time are not included, which may enrich the population and increase the response rates.
LTE LIMITATIONS: There is potential for enrichment of LTE data; unblinding patients may cause bias related to overall treatment effect.
See RINVOQ’s safety data across clinical trials
RINVOQ is indicated for the treatment of adults with moderately to severely active rheumatoid arthritis (RA) who have had an inadequate response or intolerance to one or more tumor necrosis factor (TNF) blockers.
Limitations of Use: RINVOQ is not recommended for use in combination with other Janus kinase (JAK) inhibitors, biologic disease-modifying antirheumatic drugs (bDMARDs), or with potent immunosuppressants such as azathioprine and cyclosporine.
REFERENCES:
The Disease Activity Score, 28 Joints (DAS28), C-reactive protein (CRP) variant is a measurement of rheumatoid arthritis disease activity that uses CRP as a marker of inflammation.
There are 4 components used in DAS28-CRP assessment1
DAS28-CRP is calculated using the following equation1:

DAS28 Score Interpretation2:
| SCORE | DISEASE ACTIVITY CATEGORY |
|---|---|
| 0 to <2.6 | Remission |
| 2.6 to ≤3.2 | Low disease activity (LDA) |
| >3.2 to ≤5.1 | Moderate disease activity |
| >5.1 | High disease activity |
Clinical remission does not mean drug-free remission or complete absence of disease activity.
REFERENCES:
US-RNQR-260103
SELECT-BEYOND
Adults with moderately to severely active RA who had an inadequate response or intolerance to bDMARDs1
RINVOQ is indicated for TNFi-IR patients1
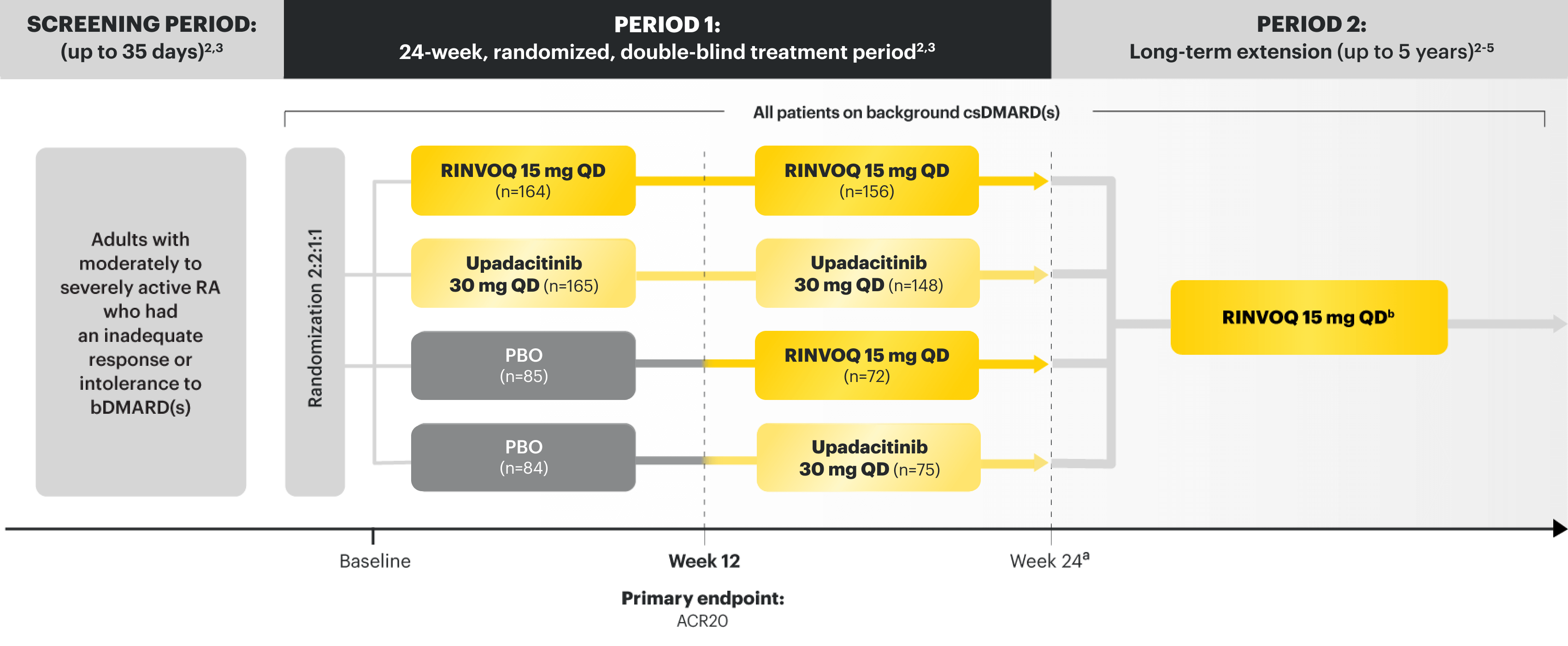
Upadacitinib 30 mg is not an approved dose.
aStarting at Week 24, initiation of or change in corticosteroids, NSAIDs, acetaminophen, and csDMARDs was permitted. Patients not achieving response criteria ≥20% improvement in SJC and TJC at 2 consecutive visits were removed from the study.4,5
bFollowing a protocol amendment, all patients in the long-term extension received UPA 15 mg QD, including those previously on UPA 30 mg.8
PRIMARY ENDPOINT1
RANKED SECONDARY ENDPOINTS6,7
At Week 12:
SELECT PRESPECIFIED NONRANKED ENDPOINTS7
DATA LIMITATIONS
Prespecified nonranked endpoints were not controlled for multiplicity; therefore, treatment differences could represent chance findings. No conclusions regarding these comparisons can be made.
BASELINE CHARACTERISTICS6
| MEAN (SD) OR n (%) | PBO + csDMARDs n=169 | RINVOQ 15 mg + csDMARDs n=164 |
|---|---|---|
| Female, n (%) | 143 (85) | 137 (84) |
| Age (years), mean (SD) | 57.6 (11.4) | 56.3 (11.3) |
| Duration since RA diagnosis (years), mean (SD) | 14.5 (9.2) | 12.4 (9.4) |
| RF+ and/or ACPA+, n (%) | 128 (76) | 131 (80) |
| csDMARD use at baseline* | ||
| - MTX alone,† n (%) | 122 (73) | 118 (73) |
| - MTX plus other csDMARD,‡ n (%) | 17 (10) | 19 (12) |
| - MTX dose§ (mg), mean (SD) | 16.6 (4.7) | 17.3 (4.6) |
| - csDMARD other than MTX, n (%) | 29 (17) | 24 (15) |
| - Missing, n | 1 | 3 |
| Prior bDMARD exposure | ||
| - 1, n (%) | 83 (49) | 86 (52) |
| - 2, n (%) | 46 (27) | 40 (24) |
| - ≥3, n (%) | 40 (24) | 38 (23) |
| Inadequate response or intolerance to ≥1 anti-TNF drug | 152 (90) | 146 (89) |
| - Lack of efficacy with ≥1 bDMARD | 159 (94) | 146 (89) |
| - Lack of efficacy with ≥1 anti–IL-6 | 30 (18) | 27 (16) |
| Oral glucocorticoid use, n (%) | 74 (44) | 83 (51) |
| - Oral glucocorticoid dosell (mg), mean (SD) | 6.3 (2.4) | 5.7 (2.4) |
| TJC68, mean (SD) | 28.5 (15.3) | 27.8 (16.3) |
| SJC66, mean (SD) | 16.3 (9.6) | 17.0 (10.8) |
| PtGA (0–100 mm VAS), mean (SD) | 66.3 (22.7) | 67.2 (19.6) |
| PhGA (0–100 mm VAS), mean (SD) | 66.9 (16.9) | 68.7 (16.6) |
| Pain (0–100 mm VAS), mean (SD) | 68.9 (21.0) | 68.2 (19.8) |
| hsCRP (mg/L), mean (SD) | 16.3 (21.1) | 16.2 (18.6) |
| DAS28-CRP, mean (SD) | 5.8 (1.0) | 5.9 (1.0) |
| HAQ-DI, mean (SD) | 1.6 (0.6) | 1.7 (0.6) |
| CDAI, mean (SD) | 41.0 (13.3) | 41.7 (13.3) |
| SDAI, mean (SD) | 42.6 (13.9) | 43.3 (13.8) |
*Oral or parenteral methotrexate (7.5–25 mg per week).
†Data available for 168 patients receiving placebo and 161 patients receiving RINVOQ 15 mg.
‡All combinations allowed except MTX and leflunomide.
§Mean MTX dose calculated only for patients receiving MTX.
‖Based on prednisone equivalent.
ACPA=anti‑citrullinated protein antibodies; ACR20=improvement of at least 20% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR50=improvement of at least 50% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR70=improvement of at least 70% in tender joint count, swollen joint count, and at least 3 other core criteria; bDMARD=biologic disease‑modifying antirheumatic drug; CDAI=Clinical Disease Activity Index; CR=clinical remission; CRP=C‑reactive protein; csDMARD=conventional synthetic disease‑modifying antirheumatic drug; DAS28-CRP=28-joint disease activity score using C-reactive protein; DAS28-ESR=28-joint disease activity score using erythrocyte sedimentation rate; ESR=erythrocyte sedimentation rate; HAQ‑DI=Health Assessment Questionnaire Disability Index; hsCRP=high‑sensitivity C‑reactive protein; IL-6=interleukin 6; IR=intolerance or inadequate response; LDA=low disease activity; MTX=methotrexate; NSAID=nonsteroidal anti‑inflammatory drug; PBO=placebo; PhGA=Physician’s Global Assessment; PtGA=patient global assessment; QD=once daily; RA=rheumatoid arthritis; RF=rheumatoid factor; SD=standard deviation; SDAI=Simplified Disease Activity Index; SF‑36 (PCS)=36‑item short form health survey physical component summary; SJC66=swollen joint count of 66 joints; TJC68=tender joint count of 68 joints; TNFi=tumor necrosis factor inhibitor; UPA=upadacitinib; VAS=visual analog scale.
REFERENCES:
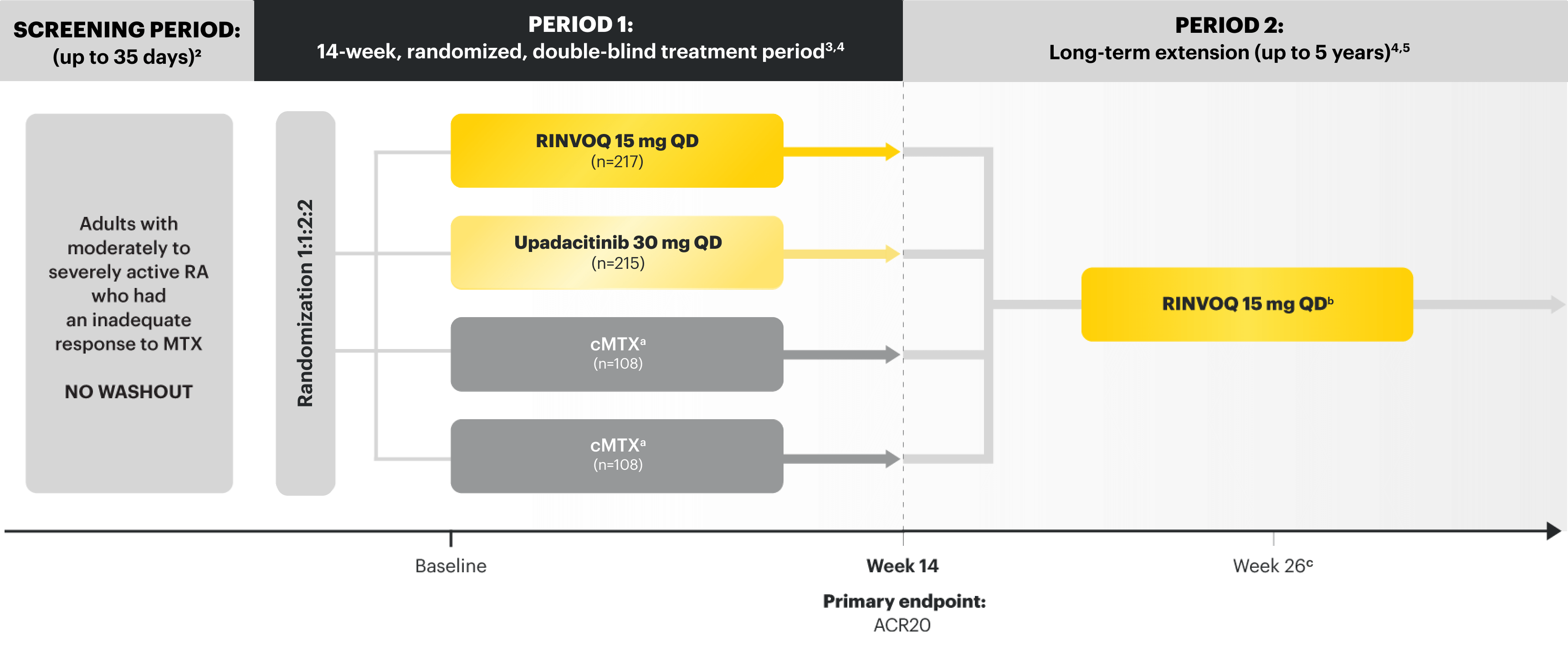
SELECT-MONOTHERAPY
Adults with moderately to severely active RA who had an inadequate response to MTX1
RINVOQ is indicated for TNFi-IR patients1
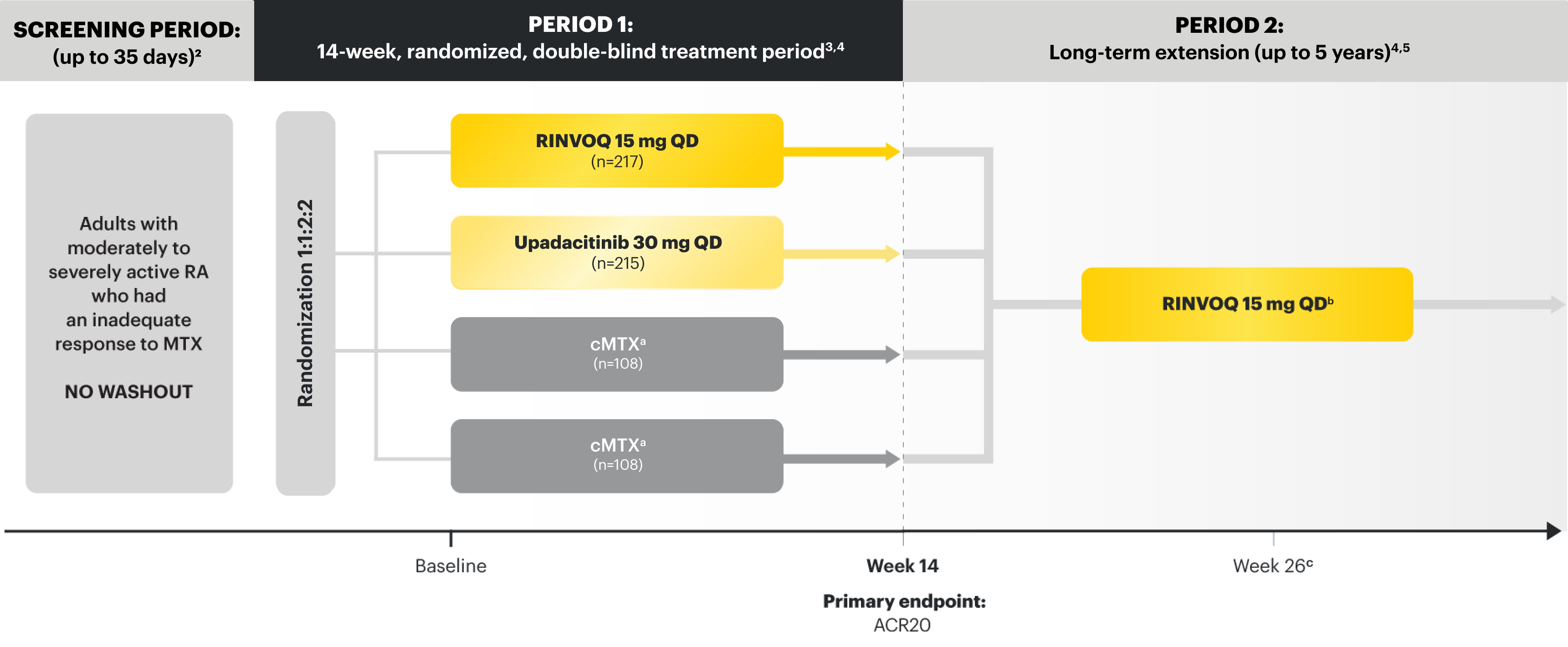
Upadacitinib 30 mg is not an approved dose.
aPatients on cMTX were randomized to receive either RINVOQ 15 mg or upadacitinib 30 mg at Week 14.3
bStarting at Week 26, patients who did not achieve CDAI ≤10 could have initiated or adjusted corticosteroids, NSAIDs, acetaminophen, or ≤2 csDMARDs. Patients who failed to show ≥20% improvement in TJC and SJC compared to baseline at 2 consecutive visits were removed from the study.4
cFollowing a protocol amendment, all patients in the long-term extension received UPA 15 mg QD, including those previously on UPA 30 mg.6
PRIMARY ENDPOINT1
RANKED SECONDARY ENDPOINTS3,7
At Week 14:
SELECT PRESPECIFIED NONRANKED ENDPOINTS3,7
DATA LIMITATIONS
Prespecified nonranked endpoints were not controlled for multiplicity; therefore, treatment differences could represent chance findings. No conclusions regarding these comparisons can be made.
BASELINE CHARACTERISTICS3
| MEAN (SD) OR N (%) | cMTX n=216 | RINVOQ 15 mg QD n=217 |
|---|---|---|
| Female, n (%) | 179 (83) | 174 (80) |
| Age (years) mean (SD) | 55.3 (11.1) | 54.5 (12.2) |
| Duration of RA diagnosis (years), mean (SD) | 5.8 (6.6) | 7.5 (8.9) |
| RF+ and/or ACPA+, n (%) | 169 (78) | 172 (79) |
| Prior MTX dose* (mg/week), mean (SD) | 16.7 (4.4) | 16.8 (4.2) |
| Prior MTX duration (years), mean (SD) | 3.3 (3.9) | 3.8 (4.8) |
| Oral glucocorticoid use, n (%) | 115 (53) | 114 (53) |
| - Oral glucocorticoid dose† (mg), mean (SD) | 6.2 (2.6) | 6.1 (2.5) |
| TJC68, mean (SD) | 25.2 (16.0) | 24.5 (15.1) |
| SJC66, mean (SD) | 16.9 (11.5) | 16.4 (10.9) |
| PtGA (0–100 mm VAS), mean (SD) | 59.6 (21.8) | 62.2 (22.3) |
| PhGA (0–100 mm VAS), mean (SD) | 62.1 (17.5) | 65.7 (18.5) |
| Pain (0–100 mm VAS), mean (SD) | 62.5 (21.3) | 62.3 (22.5) |
| hsCRP (mg/L), mean (SD) | 14.5 (17.3) | 14.0 (16.5) |
| DAS28-CRP, mean (SD) | 5.6 (1.0) | 5.6 (0.9) |
| HAQ-DI, mean (SD) | 1.5 (0.7) | 1.5 (0.7) |
| CDAI, mean (SD) | 37.8 (14.4) | 38.0 (13.1) |
| SDAI, mean (SD) | 39.2 (14.6) | 39.4 (13.4) |
*Prior to receiving study drug. In the control arm, patients continued prior MTX dose as blinded study drug.3
†Prednisone equivalent.
ACPA=anti‑citrullinated protein antibody; ACR=American College of Rheumatology; ACR20=improvement of at least 20% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR50=improvement of at least 50% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR70=improvement of at least 70% in tender joint count, swollen joint count, and at least 3 other core criteria; CDAI=Clinical Disease Activity Index; cMTX=continuous methotrexate; csDMARD=conventional synthetic disease‑modifying antirheumatic drug; CR=clinical remission; CRP=C‑reactive protein; DAS28-CRP=28-joint disease activity score using C-reactive protein; DAS28-ESR=28-joint disease activity score using erythrocyte sedimentation rate; ESR=erythrocyte sedimentation rate; HAQ‑DI=Health Assessment Questionnaire Disability Index; hsCRP=high-sensitivity C‑reactive protein; IR=intolerance or inadequate response; LDA=low disease activity; MTX=methotrexate; NSAID=nonsteroidal anti‑inflammatory drug; PhGA=Physician’s Global Assessment; PtGA=patient global assessment; QD=once daily; RA=rheumatoid arthritis; RF=rheumatoid factor; SD=standard deviation; SDAI=Simplified Disease Activity Index; SF‑36 (PCS)=36-item short form health survey physical component summary; SJC66=swollen joint count of 66 joints; TJC68=tender joint count of 68 joints; TNFi=tumor necrosis factor inhibitor; UPA=upadacitinib; VAS=visual analog scale.
REFERENCES:
US-RNQR-260103
SELECT-BEYOND
Adults with moderately to severely active RA who had an inadequate response or intolerance to bDMARDs1
RINVOQ is indicated for TNFi-IR patients1
Upadacitinib 30 mg is not an approved dose.
aStarting at Week 24, initiation of or change in corticosteroids, NSAIDs, acetaminophen, and csDMARDs was permitted. Patients not achieving response criteria ≥20% improvement in SJC and TJC at 2 consecutive visits were removed from the study.4,5
bFollowing a protocol amendment, all patients in the long-term extension received UPA 15 mg QD, including those previously on UPA 30 mg.8
PRIMARY ENDPOINT1
RANKED SECONDARY ENDPOINTS6,7
At Week 12:
SELECT PRESPECIFIED NON-RANKED ENDPOINTS7
DATA LIMITATIONS
Prespecified non-ranked endpoints were not controlled for multiplicity; therefore, treatment differences could represent chance findings. No conclusions regarding these comparisons can be made.
BASELINE CHARACTERISTICS6
| MEAN (SD) OR n (%) | PBO + csDMARDs n=169 | RINVOQ 15 mg + csDMARDs n=164 |
|---|---|---|
| Female, n (%) | 143 (85) | 137 (84) |
| Age (years), mean (SD) | 57.6 (11.4) | 56.3 (11.3) |
| Duration since RA diagnosis (years), mean (SD) | 14.5 (9.2) | 12.4 (9.4) |
| RF+ and/or ACPA+, n (%) | 128 (76) | 131 (80) |
| csDMARD use at baseline* | ||
| - MTX alone,† n (%) | 122 (73) | 118 (73) |
| - MTX plus other csDMARD,‡ n (%) | 17 (10) | 19 (12) |
| - MTX dose§ (mg), mean (SD) | 16.6 (4.7) | 17.3 (4.6) |
| - csDMARD other than MTX, n (%) | 29 (17) | 24 (15) |
| - Missing, n | 1 | 3 |
| Prior bDMARD exposure | ||
| - 1, n (%) | 83 (49) | 86 (52) |
| - 2, n (%) | 46 (27) | 40 (24) |
| - ≥3, n (%) | 40 (24) | 38 (23) |
| Inadequate response or intolerance to ≥1 anti-TNF drug | 152 (90) | 146 (89) |
| - Lack of efficacy with ≥1 bDMARD | 159 (94) | 146 (89) |
| - Lack of efficacy with ≥1 anti-IL-6 | 30 (18) | 27 (16) |
| Oral glucocorticoid use, n (%) | 74 (44) | 83 (51) |
| - Oral glucocorticoid dosell (mg), mean (SD) | 6.3 (2.4) | 5.7 (2.4) |
| TJC68, mean (SD) | 28.5 (15.3) | 27.8 (16.3) |
| SJC66, mean (SD) | 16.3 (9.6) | 17.0 (10.8) |
| PtGA (0-100 mm VAS), mean (SD) | 66.3 (22.7) | 67.2 (19.6) |
| PhGA (0-100 mm VAS), mean (SD) | 66.9 (16.9) | 68.7 (16.6) |
| Pain (0-100 mm VAS), mean (SD) | 68.9 (21.0) | 68.2 (19.8) |
| hsCRP (mg/L), mean (SD) | 16.3 (21.1) | 16.2 (18.6) |
| DAS28-CRP, mean (SD) | 5.8 (1.0) | 5.9 (1.0) |
| HAQ-DI, mean (SD) | 1.6 (0.6) | 1.7 (0.6) |
| CDAI, mean (SD) | 41.0 (13.3) | 41.7 (13.3) |
| SDAI, mean (SD) | 42.6 (13.9) | 43.3 (13.8) |
*Oral or parenteral methotrexate (7.5-25 mg per week).
†Data available for 168 patients receiving placebo and 161 patients receiving RINVOQ 15 mg.
‡All combinations allowed except MTX and leflunomide.
§Mean MTX dose calculated only for patients receiving MTX.
‖Based on prednisone equivalent.
ACPA=anti‑citrullinated protein antibodies; ACR20=improvement of at least 20% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR50=improvement of at least 50% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR70=improvement of at least 70% in tender joint count, swollen joint count, and at least 3 other core criteria; bDMARD=biologic disease‑modifying antirheumatic drug; CDAI=Clinical Disease Activity Index; CR=clinical remission; CRP=C‑reactive protein; csDMARD=conventional synthetic disease‑modifying antirheumatic drug; DAS28-CRP=28-joint disease activity score using C-reactive protein; DAS28-ESR=28-joint disease activity score using erythrocyte sedimentation rate; ESR=erythrocyte sedimentation rate; HAQ‑DI=Health Assessment Questionnaire Disability Index; hsCRP=high‑sensitivity C‑reactive protein; IL-6=interleukin 6; IR=intolerance or inadequate response; LDA=low disease activity; MTX=methotrexate; NSAID=nonsteroidal anti‑inflammatory drug; PBO=placebo; PhGA=physician’s global assessment of disease activity; PtGA=patient’s global assessment of disease activity; QD=once daily; RA=rheumatoid arthritis; RF=rheumatoid factor; SD=standard deviation; SDAI=Simplified Disease Activity Index; SF‑36 (PCS)=36‑item short form health survey physical component summary; SJC66=swollen joint count of 66 joints; TJC68=tender joint count of 68 joints; TNFi=tumor necrosis factor inhibitor; UPA=upadacitinib; VAS=visual analog scale.
REFERENCES:
SELECT-MONOTHERAPY
Adults with moderately to severely active RA who had an inadequate response to MTX1
RINVOQ is indicated for TNFi-IR patients1
Upadacitinib 30 mg is not an approved dose.
aPatients on cMTX were randomized to receive either RINVOQ 15 mg or upadacitinib 30 mg at Week 14.3
bStarting at Week 26, patients who did not achieve CDAI ≤10 could have initiated or adjusted corticosteroids, NSAIDs, acetaminophen, or ≤2 csDMARDs. Patients who failed to show ≥20% improvement in TJC and SJC compared to baseline at 2 consecutive visits were removed from the study.4
cFollowing a protocol amendment, all patients in the long-term extension received UPA 15 mg QD, including those previously on UPA 30 mg.6
PRIMARY ENDPOINT1
RANKED SECONDARY ENDPOINTS3,7
At Week 14:
SELECT PRESPECIFIED NON-RANKED ENDPOINTS3,7
DATA LIMITATIONS
Prespecified non-ranked endpoints were not controlled for multiplicity; therefore, treatment differences could represent chance findings. No conclusions regarding these comparisons can be made.
BASELINE CHARACTERISTICS3
| MEAN (SD) OR N (%) | cMTX n=216 | RINVOQ 15 mg QD n=217 |
|---|---|---|
| Female, n (%) | 179 (83) | 174 (80) |
| Age (years) mean (SD) | 55.3 (11.1) | 54.5 (12.2) |
| Duration of RA diagnosis (years), mean (SD) | 5.8 (6.6) | 7.5 (8.9) |
| RF+ and/or ACPA+, n (%) | 169 (78) | 172 (79) |
| Prior MTX dose* (mg/week), mean (SD) | 16.7 (4.4) | 16.8 (4.2) |
| Prior MTX duration (years), mean (SD) | 3.3 (3.9) | 3.8 (4.8) |
| Oral glucocorticoid use, n (%) | 115 (53) | 114 (53) |
| - Oral glucocorticoid dose† (mg), mean (SD) | 6.2 (2.6) | 6.1 (2.5) |
| TJC68, mean (SD) | 25.2 (16.0) | 24.5 (15.1) |
| SJC66, mean (SD) | 16.9 (11.5) | 16.4 (10.9) |
| PtGA (0-100 mm VAS), mean (SD) | 59.6 (21.8) | 62.2 (22.3) |
| PhGA (0-100 mm VAS), mean (SD) | 62.1 (17.5) | 65.7 (18.5) |
| Pain (0-100 mm VAS), mean (SD) | 62.5 (21.3) | 62.3 (22.5) |
| hsCRP (mg/L), mean (SD) | 14.5 (17.3) | 14.0 (16.5) |
| DAS28-CRP, mean (SD) | 5.6 (1.0) | 5.6 (0.9) |
| HAQ-DI, mean (SD) | 1.5 (0.7) | 1.5 (0.7) |
| CDAI, mean (SD) | 37.8 (14.4) | 38.0 (13.1) |
| SDAI, mean (SD) | 39.2 (14.6) | 39.4 (13.4) |
*Prior to receiving study drug. In the control arm, patients continued prior MTX dose as blinded study drug.3
†Prednisone equivalent.
ACPA=anti‑citrullinated protein antibody; ACR=American College of Rheumatology; ACR20=improvement of at least 20% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR50=improvement of at least 50% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR70=improvement of at least 70% in tender joint count, swollen joint count, and at least 3 other core criteria; CDAI=Clinical Disease Activity Index; cMTX=continuous methotrexate; csDMARD=conventional synthetic disease‑modifying antirheumatic drug; CR=clinical remission; CRP=C‑reactive protein; DAS28-CRP=28-joint disease activity score using C-reactive protein; DAS28-ESR=28-joint disease activity score using erythrocyte sedimentation rate; ESR=erythrocyte sedimentation rate; HAQ‑DI=Health Assessment Questionnaire Disability Index; hsCRP=high-sensitivity C‑reactive protein; IR=intolerance or inadequate response; LDA=low disease activity; MTX=methotrexate; NSAID=nonsteroidal anti‑inflammatory drug; PhGA=physician’s global assessment of disease activity; PtGA=patient’s global assessment of disease activity; QD=once daily; RA=rheumatoid arthritis; RF=rheumatoid factor; SD=standard deviation; SDAI=Simplified Disease Activity Index; SF‑36 (PCS)=36-item short form health survey physical component summary; SJC66=swollen joint count of 66 joints; TJC68=tender joint count of 68 joints; TNFi=tumor necrosis factor inhibitor; UPA=upadacitinib; VAS=visual analog scale.
REFERENCES:
SELECT-BEYOND
Adults with moderately to severely active RA who had an inadequate response or intolerance to bDMARDs1
RINVOQ is indicated for TNFi-IR patients1

Upadacitinib 30 mg is not an approved dose.
aStarting at Week 24, initiation of or change in corticosteroids, NSAIDs, acetaminophen, and csDMARDs was permitted. Patients not achieving response criteria ≥20% improvement in SJC and TJC at 2 consecutive visits were removed from the study.4,5
bFollowing a protocol amendment, all patients in the long-term extension received UPA 15 mg QD, including those previously on UPA 30 mg.8
PRIMARY ENDPOINT1
RANKED SECONDARY ENDPOINTS6,7
At Week 12:
SELECT PRESPECIFIED NONRANKED ENDPOINTS7
DATA LIMITATIONS
Prespecified nonranked endpoints were not controlled for multiplicity; therefore, treatment differences could represent chance findings. No conclusions regarding these comparisons can be made.
BASELINE CHARACTERISTICS6
| MEAN (SD) OR N (%) | PBO + csDMARDs n=169 | RINVOQ 15 mg + csDMARDs n=164 |
|---|---|---|
| Female, n (%) | 143 (85) | 137 (84) |
| Age (years), mean (SD) | 57.6 (11.4) | 56.3 (11.3) |
| Duration since RA diagnosis (years), mean (SD) | 14.5 (9.2) | 12.4 (9.4) |
| RF+ and/or ACPA+, n (%) | 128 (76) | 131 (80) |
| csDMARD use at baseline* | ||
| - MTX alone,† n (%) | 122 (73) | 118 (73) |
| - MTX plus other csDMARD,‡ n (%) | 17 (10) | 19 (12) |
| - MTX dose§ (mg), mean (SD) | 16.6 (4.7) | 17.3 (4.6) |
| - csDMARD other than MTX, n (%) | 29 (17) | 24 (15) |
| - Missing, n | 1 | 3 |
| Prior bDMARD exposure | ||
| - 1, n (%) | 83 (49) | 86 (52) |
| - 2, n (%) | 46 (27) | 40 (24) |
| - ≥3, n (%) | 40 (24) | 38 (23) |
| Inadequate response or intolerance to ≥1 anti-TNF drug | 152 (90) | 146 (89) |
| - Lack of efficacy with ≥1 bDMARD | 159 (94) | 146 (89) |
| - Lack of efficacy with ≥1 anti–IL-6 | 30 (18) | 27 (16) |
| Oral glucocorticoid use, n (%) | 74 (44) | 83 (51) |
| - Oral glucocorticoid dosell (mg), mean (SD) | 6.3 (2.4) | 5.7 (2.4) |
| TJC68, mean (SD) | 28.5 (15.3) | 27.8 (16.3) |
| SJC66, mean (SD) | 16.3 (9.6) | 17.0 (10.8) |
| PtGA (0–100 mm VAS), mean (SD) | 66.3 (22.7) | 67.2 (19.6) |
| PhGA (0–100 mm VAS), mean (SD) | 66.9 (16.9) | 68.7 (16.6) |
| Pain (0–100 mm VAS), mean (SD) | 68.9 (21.0) | 68.2 (19.8) |
| hsCRP (mg/L), mean (SD) | 16.3 (21.1) | 16.2 (18.6) |
| DAS28-CRP, mean (SD) | 5.8 (1.0) | 5.9 (1.0) |
| HAQ-DI, mean (SD) | 1.6 (0.6) | 1.7 (0.6) |
| CDAI, mean (SD) | 41.0 (13.3) | 41.7 (13.3) |
| SDAI, mean (SD) | 42.6 (13.9) | 43.3 (13.8) |
*Oral or parenteral methotrexate (7.5–25 mg per week).
†Data available for 168 patients receiving placebo and 161 patients receiving RINVOQ 15 mg.
‡All combinations allowed except MTX and leflunomide.
§Mean MTX dose calculated only for patients receiving MTX.
‖Based on prednisone equivalent.
ACPA=anti‑citrullinated protein antibodies; ACR20=improvement of at least 20% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR50=improvement of at least 50% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR70=improvement of at least 70% in tender joint count, swollen joint count, and at least 3 other core criteria; bDMARD=biologic disease‑modifying antirheumatic drug; CDAI=Clinical Disease Activity Index; CR=clinical remission; CRP=C‑reactive protein; csDMARD=conventional synthetic disease‑modifying antirheumatic drug; DAS28-CRP=28-joint disease activity score using C-reactive protein; DAS28-ESR=28-joint disease activity score using erythrocyte sedimentation rate; ESR=erythrocyte sedimentation rate; HAQ‑DI=Health Assessment Questionnaire Disability Index; hsCRP=high‑sensitivity C‑reactive protein; IL-6=interleukin 6; IR=intolerance or inadequate response; LDA=low disease activity; MTX=methotrexate; NSAID=nonsteroidal anti‑inflammatory drug; PBO=placebo; PhGA=Physician’s Global Assessment; PtGA=patient global assessment; QD=once daily; RA=rheumatoid arthritis; RF=rheumatoid factor; SD=standard deviation; SDAI=Simplified Disease Activity Index; SF‑36 (PCS)=36‑item short form health survey physical component summary; SJC66=swollen joint count of 66 joints; TJC68=tender joint count of 68 joints; TNFi=tumor necrosis factor inhibitor; UPA=upadacitinib; VAS=visual analog scale.
REFERENCES:
SELECT-COMPARE
Adults with moderately to severely active RA who had an inadequate response to MTX1
RINVOQ is indicated for TNFi-IR patients1
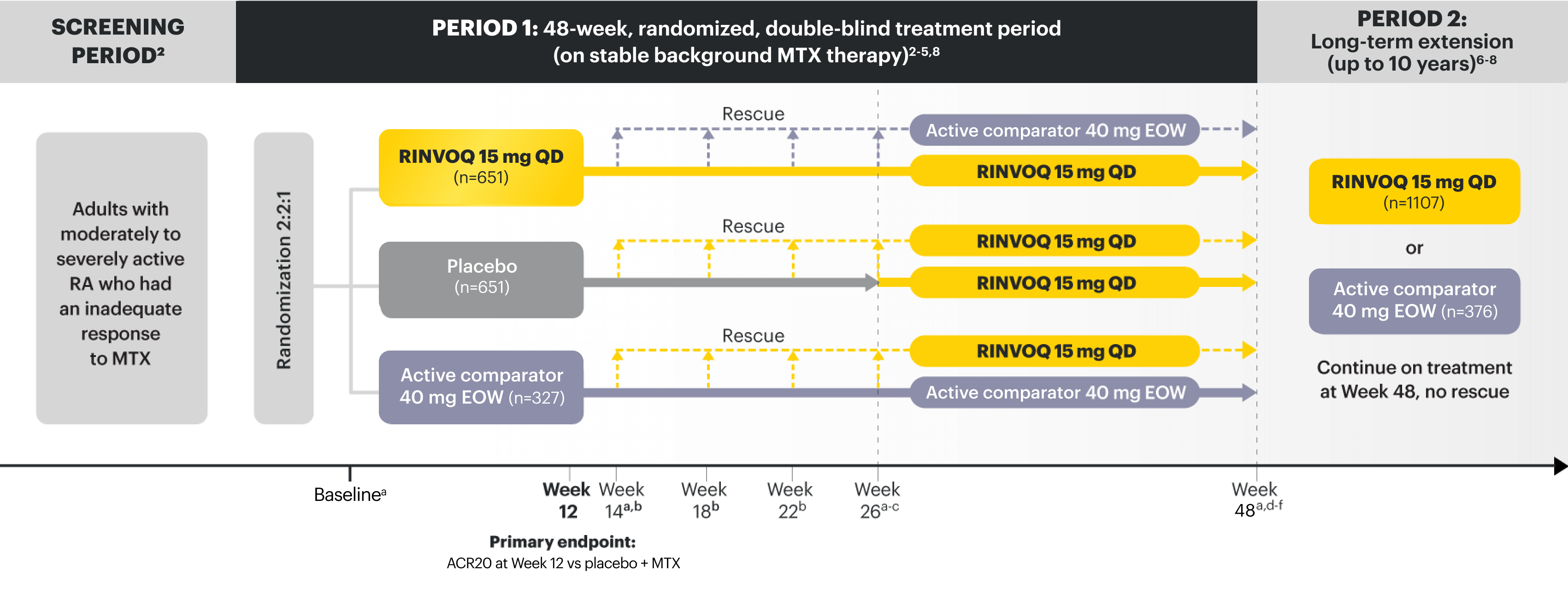
aX-ray imaging was performed at these time points; Week 14 for nonresponder patients, who were rescued.2,3
bRescue criteria: At Weeks 14, 18, and 22, if <20% improvement in TJC and SJC vs baseline; at Week 26, all remaining PBO patients were switched to RINVOQ, and patients receiving RINVOQ or active comparator were switched to active comparator or RINVOQ, respectively, if CDAI >10.2
cStarting at Week 26, initiation or change in background RA medication(s), including corticosteroids, NSAIDs, or acetaminophen was permitted.4
dStarting at Week 48, patients who failed to show ≥20% improvement in TJC and SJC compared to baseline at 2 consecutive visits were removed from the study.5
eAt Week 48, initiation or change in csDMARDs was allowed; however, not all patients received background MTX.5
fPatients continued treatment with UPA or active comparator in a blinded manner until the last patient completed the Week 48 visit and received open-label treatment thereafter.8
PRIMARY ENDPOINT1
SELECT RANKED SECONDARY ENDPOINTS2
At Week 12 vs placebo + MTX:
At Week 12 vs active comparator + MTX:
At Week 26 vs placebo + MTX:
SELECT PRESPECIFIED NONRANKED ENDPOINTS3,9,10
DATA LIMITATIONS
Prespecified nonranked endpoints were not controlled for multiplicity; therefore, treatment differences could represent chance findings. No conclusions regarding these comparisons can be made.
SELECT-COMPARE was not designed to evaluate the efficacy of active comparator + MTX vs placebo + MTX. No conclusions regarding this comparison can be made.
BASELINE CHARACTERISTICS3
| MEAN (SD) OR N (%) | PBO + MTX n=651 | RINVOQ 15 mg QD + MTX n=651 |
|---|---|---|
| Female, n (%) | 512 (79) | 521 (80) |
| Age (years), mean (SD) | 54 (12) | 54 (12) |
| Duration since RA diagnosis (years), mean (SD) | 8 (8) | 8 (8) |
| RF+ and/or anti-CCP+, n (%) | 571 (88) | 566 (87) |
| MTX dose (mg/week), mean (SD) | 16.8 (3.8) | 17.0 (4.2) |
| Prior bDMARD use, n (%) | 63 (10) | 54 (8) |
| Oral glucocorticoid use, n (%) | 392 (60) | 388 (60) |
| - Dose (mg),* mean (SD) | 6.3 (2.4) | 6.2 (2.3) |
| TJC68, mean (SD) | 26 (14) | 26 (15) |
| SJC66, mean (SD) | 16 (9) | 17 (10) |
| PtGA (0–100 mm VAS), mean (SD) | 64 (21) | 64 (22) |
| PhGA (0–100 mm VAS), mean (SD) | 66 (18) | 66 (17) |
| Pain (0–100 mm VAS), mean (SD) | 65 (21) | 66 (21) |
| hsCRP (mg/L), mean (SD) | 18 (22) | 18 (22) |
| DAS28-CRP, mean (SD) | 5.8 (0.9) | 5.8 (1.0) |
| HAQ-DI, mean (SD) | 1.6 (0.6) | 1.6 (0.6) |
| CDAI, mean (SD) | 40 (13) | 40 (13) |
| SDAI, mean (SD) | 41.8 (13.3) | 41.5 (13.6) |
| mTSS, mean (SD) | 36 (52) | 34 (50) |
| - JE score, mean (SD) | 17 (27) | 17 (26) |
| - JSN score, mean (SD) | 19 (26) | 18 (25) |
*Based on prednisone equivalent.
ACPA=anti-citrullinated protein antibody; ACR=American College of Rheumatology; ACR20=improvement of at least 20% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR50=improvement of at least 50% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR70=improvement of at least 70% in tender joint count, swollen joint count, and at least 3 other core criteria; bDMARD=biologic disease‑modifying antirheumatic drug; CCP=cyclic citrullinated peptide; CDAI=Clinical Disease Activity Index; CR=clinical remission; CRP=C‑reactive protein; csDMARD=conventional synthetic disease-modifying antirheumatic drug; DAS28-CRP=28-joint disease activity score using C-reactive protein; DAS28-ESR=28-joint disease activity score using erythrocyte sedimentation rate; EOW=every other week; ESR=erythrocyte sedimentation rate; HAQ‑DI=Health Assessment Questionnaire Disability Index; hsCRP=high-sensitivity C‑reactive protein; IR=intolerance or inadequate response; JE=joint erosion; JSN=joint space narrowing; LDA=low disease activity; mTSS=modified total Sharp score; MTX=methotrexate; NSAID=nonsteroidal anti-inflammatory drug; PBO=placebo; PhGA=Physician's Global Assessment; PtGA=patient global assessment; QD=once per day; RA=rheumatoid arthritis; RF=rheumatoid factor; SD=standard deviation; SDAI=Simplified Disease Activity Index; SF‑36 (PCS)=36-item short form health survey physical component summary; SJC66=swollen joint count of 66 joints; TJC68=tender joint count of 68 joints; TNFi=tumor necrosis factor inhibitor; UPA=upadacitinib; VAS=visual analog scale.
REFERENCES:
SELECT-MONOTHERAPY
Adults with moderately to severely active RA who had an inadequate response to MTX1
RINVOQ is indicated for TNFi-IR patients1
Upadacitinib 30 mg is not an approved dose.
aPatients on cMTX were randomized to receive either RINVOQ 15 mg or upadacitinib 30 mg at Week 14.3
bStarting at Week 26, patients who did not achieve CDAI ≤10 could have initiated or adjusted corticosteroids, NSAIDs, acetaminophen, or ≤2 csDMARDs. Patients who failed to show ≥20% improvement in TJC and SJC compared to baseline at 2 consecutive visits were removed from the study.5
cFollowing a protocol amendment, all patients in the long-term extension received UPA 15 mg QD, including those previously on UPA 30 mg.4
PRIMARY ENDPOINT1
RANKED SECONDARY ENDPOINTS3,6
At Week 14:
SELECT PRESPECIFIED NONRANKED ENDPOINTS3,6
DATA LIMITATIONS
Prespecified nonranked endpoints were not controlled for multiplicity; therefore, treatment differences could represent chance findings. No conclusions regarding these comparisons can be made.
BASELINE CHARACTERISTICS3
| MEAN (SD) OR N (%) | cMTX n=216 | RINVOQ 15 mg QD n=217 |
|---|---|---|
| Female, n (%) | 179 (83) | 174 (80) |
| Age (years), mean (SD) | 55.3 (11.1) | 54.5 (12.2) |
| Duration since RA diagnosis (years), mean (SD) | 5.8 (6.6) | 7.5 (8.9) |
| RF+ and/or ACPA+, n (%) | 169 (78) | 172 (79) |
| Prior MTX dose* (mg/week), mean (SD) | 16.7 (4.4) | 16.8 (4.2) |
| Prior MTX duration (years), mean (SD) | 3.3 (3.9) | 3.8 (4.8) |
| Oral glucocorticoid use, n (%) | 115 (53) | 114 (53) |
| - Oral glucocorticoid dose† (mg), mean (SD) | 6.2 (2.6) | 6.1 (2.5) |
| TJC68, mean (SD) | 25.2 (16.0) | 24.5 (15.1) |
| SJC66, mean (SD) | 16.9 (11.5) | 16.4 (10.9) |
| PtGA (0–100 mm VAS), mean (SD) | 59.6 (21.8) | 62.2 (22.3) |
| PhGA (0–100 mm VAS), mean (SD) | 62.1 (17.5) | 65.7 (18.5) |
| Pain (0–100 mm VAS), mean (SD) | 62.5 (21.3) | 62.3 (22.5) |
| hsCRP (mg/L), mean (SD) | 14.5 (17.3) | 14.0 (16.5) |
| DAS28-CRP, mean (SD) | 5.6 (1.0) | 5.6 (0.9) |
| HAQ-DI, mean (SD) | 1.5 (0.7) | 1.5 (0.7) |
| CDAI, mean (SD) | 37.8 (14.4) | 38.0 (13.1) |
| SDAI, mean (SD) | 39.2 (14.6) | 39.4 (13.4) |
*Prior to receiving study drug. In the control arm, patients continued prior MTX dose as blinded study drug.3
†Prednisone equivalent.
ACPA=anti‑citrullinated protein antibody; ACR=American College of Rheumatology; ACR20=improvement of at least 20% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR50=improvement of at least 50% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR70=improvement of at least 70% in tender joint count, swollen joint count, and at least 3 other core criteria; CDAI=Clinical Disease Activity Index; cMTX=continuous methotrexate; csDMARD=conventional synthetic disease‑modifying antirheumatic drug; CR=clinical remission; CRP=C‑reactive protein; DAS28-CRP=28-joint disease activity score using C-reactive protein; DAS28-ESR=28-joint disease activity score using erythrocyte sedimentation rate; ESR=erythrocyte sedimentation rate; HAQ‑DI=Health Assessment Questionnaire Disability Index; hsCRP=high-sensitivity C‑reactive protein; IR=intolerance or inadequate response; LDA=low disease activity; MTX=methotrexate; NSAID=nonsteroidal anti‑inflammatory drug; PhGA=Physician’s Global Assessment; PtGA=patient global assessment; QD=once daily; RA=rheumatoid arthritis; RF=rheumatoid factor; SD=standard deviation; SDAI=Simplified Disease Activity Index; SF‑36 (PCS)=36-item short form health survey physical component summary; SJC66=swollen joint count of 66 joints; TJC68=tender joint count of 68 joints; TNFi=tumor necrosis factor inhibitor; UPA=upadacitinib; VAS=visual analog scale.
REFERENCES:
SELECT-SWITCH
Head-to-head study powered to evaluate superiority of RINVOQ vs HUMIRA (adalimumab) in RA patients who had inadequate response or intolerance to 1 TNFi2
A 12-week, randomized, double-blind, active-comparator–controlled study of 491 adult patients with moderate to severe RA who did not respond to 1 TNFi (non-adalimumab). Designed to evaluate superiority of continuing TNFi therapy with HUMIRA (adalimumab) vs switching to RINVOQ (upadacitinib).

PRIMARY ENDPOINT2
SELECT RANKED SECONDARY ENDPOINTS2
At Week 12 vs HUMIRA:
SELECT PRESPECIFIED NONRANKED ENDPOINTS2
At all visits:
| MEAN (SD) Unless otherwise stated |
RINVOQ 15 mg QD + MTX (n=245) | HUMIRA 40 mg EOW + MTX n=246* |
|---|---|---|
| Parameter | ||
| Age (years) | 55.3 (12.7) | 55.9 (12.5) |
| Age ≥65 years, n (%) | 57 (23.3) | 72 (29.3) |
| Female, n (%) | 189 (77.1) | 191 (77.6) |
| BMI (kg/m2) | 29.4 (6.5) | 28.8 (7.0) |
| RA duration since diagnosis (years) | 10.1 (8.5) (n=244) | 10.3 (9.3) |
| Disease Characteristics | ||
| DAS28-CRP | 5.7 (0.8) (n=235) | 5.7 (0.8) (n=236) |
| DAS28-ESR | 6.3 (0.9) (n=234) | 6.4 (0.9) (n=235) |
| TJC68 | 22.4 (12.3) | 22.8 (12.6) |
| SJC66 | 15.5 (6.6) | 15.9 (8.3) |
| hsCRP (mg/L) | 16.8 (25.4) (n=245) | 14.0 (17.6) |
| ESR (mm/hr) | 37.1 (23.4) (n=243) | 38.9 (24.4) (n=245) |
| PtGA (0–10 NRS) | 7.1 (1.9) (n=235) | 7.4 (1.9) (n=236) |
| PhGA (0–10 NRS) | 7.0 (1.6) | 6.9 (1.6) |
| Pain (0–10 NRS) | 7.4 (1.9) | 7.4 (1.9) (n=232) |
| HAQ-DI | 1.6 (0.6) (n=234) | 1.6 (0.6) (n=234) |
| FACIT-Fatigue | 26.8 (11.5) (n=234) | 26.8 (10.5) (n=233) |
| Concomitant Therapies | ||
| Patients receiving oral corticosteroid at baseline, n (%) | 99 (40.4) | 100 (40.7) |
| Oral steroid dose (prednisone equivalent) at baseline (mg/day) | 6.4 (2.7) (n=99) | 6.7 (3.2) (n=100) |
| MTX dose at baseline (mg/week), median | 15.0 | 15.0 (n=245) |
| NSAIDs | 128 (52.2) | 111 (45.1) |
| Patient History, n (%) | ||
| HZ vaccination | 35 (14.6) | 31 (12.8) |
| History of VTE | 2 (0.8) | 2 (0.8) |
| History of CV event | 18 (7.3) | 11 (4.5) |
| Number of CV risk factorsa, n (%) | ||
| 0 | 72 (29.4) | 65 (26.4) |
| 1 | 94 (38.4) | 107 (43.5) |
| 2 | 58 (23.7) | 61 (24.8) |
| 3+ | 21 (8.6) | 13 (5.3) |
| CV risk factors at baseline, n (%) | ||
| Hypertension | 90 (36.7) | 85 (34.6) |
| Diabetes mellitus | 6 (2.4) | 2 (0.8) |
| History of tobacco/nicotine use (current/former) | 89 (36.3) | 77 (31.3) |
| Elevated LDL-Cb | 42 (17.1) | 65 (26.4) |
| Low HDL-Cc | 36 (14.7) | 32 (13.0) |
| Reason for discontinuation of prior TNFi, n (%) | ||
| Intolerance | 25 (10.2) | 27 (11.0) |
| Inadequate response | 220 (89.8) | 219 (89.0) |
| Type of inadequate response to prior TNFi, n (%) | ||
| Primary nonresponder | 121 (55.8) | 115 (54.0) |
| Secondary nonresponder | 96 (44.2) | 98 (46.0) |
| Missing | 3 | 6 |
| Prior TNFi administered, n (%) | ||
| Etanercept | 165 (67.3) | 170 (69.1) |
| Certolizumab | 40 (16.3) | 35 (14.2) |
| Golimumab | 24 (9.8) | 21 (8.5) |
| Infliximab | 15 (6.1) | 13 (5.3) |
| Adalimumab† | 0 | 1 (0.4) |
*Patients entered the study while receiving a stable dose of MTX (15–25 mg/week). MTX was not considered an ancillary drug in the study.2
†Protocol deviations.2
aCV risk factors included CV event, hypertension, diabetes mellitus, tobacco/nicotine use, elevated LDL-C, and lowered HDL‑C.
b≥3.36 mmol/L (ie, >129.9 mg/dL).
c<1.034 mmol/L (ie, <18.6 mg/dL).
ACR=American College of Rheumatology; BMI=body mass index; CDAI=Clinical Disease Activity Index; CRP=C-reactive protein; CV=cardiovascular; DAS28-CRP=Disease Activity Score in 28 joints using C-reactive protein; DAS28-ESR=28-joint Disease Activity Score using erythrocyte sedimentation rate; EOW=every other week; ESR=erythrocyte sedimentation rate; FACIT-Fatigue=Functional Assessment of Chronic Illness Therapy-Fatigue; HAQ-DI=Health Assessment Questionnaire-Disability Index; HDL-C=high-density lipoprotein cholesterol; hsCRP=high-sensitivity C-reactive protein; HZ=herpes zoster; IR=intolerance or inadequate response; LDA=low disease activity; LDL-C=low-density lipoprotein cholesterol; MACE=major adverse cardiovascular event; MTX=methotrexate; NSAID=nonsteroidal anti-inflammatory drug; PhGA=Physician's Global Assessment; PtGA=patient global assessment; primary nonresponder=patient who did not respond to prior TNFi treatment; QD=once daily; RA=rheumatoid arthritis; SC=subcutaneous; SD=standard deviation; SDAI=Simplified Disease Activity Index; secondary nonresponder=patient who initially responded to prior TNFi treatment but lost response over time; SJC66=swollen joint count of 66 joints; TJC68=tender joint count of 68 joints; TNFi=tumor necrosis factor inhibitor; VTE=venous thromboembolism.
REFERENCES:
SELECT-EARLY
Adults with moderately to severely active RA who were MTX‑naïve1
RINVOQ is indicated for TNFi-IR patients1

Upadacitinib 30 mg is not an approved dose.
aInitially 947 patients were randomized in the study, but 2 patients were never dosed.
bX-ray images of hands and feet obtained at these time points.2
cStarting at Week 12, patients with ≤20% improvement in TJC and SJC compared to baseline at 2 consecutive visits continued blinded therapy and optimized background RA medications (corticosteroids, NSAIDs, and/or low‑potency analgesics).3,4
dAt Week 26, patients with CDAI ≤2.8 continued their original study drug; background medications (NSAIDs, corticosteroids, and/or low‑potency analgesics, and csDMARDs) were optimized in patients with CDAI >2.8 but ≥20% improvement in TJC and SJC; among patients with CDAI >2.8 and <20% improvement in TJC and SJC, RINVOQ 15 mg or upadacitinib 30 mg were added by re‑randomization according to 1:1 ratio for those initially randomized to MTX, and MTX was added for those initially randomized to RINVOQ 15 mg or upadacitinib 30 mg.2,5
eStarting at Week 48, patients who did not achieve ≥20% improvement in both TJC and SJC at 2 consecutive visits were removed from the study. Initiation of or change in background RA medications (NSAIDs, corticosteroids, low-potency analgesics, and csDMARDs; not all patients received background MTX) is allowed at anytime during Period 2.6
fFollowing a protocol amendment, all patients in the long-term extension who were previously receiving UPA 30 mg received RINVOQ 15 mg.11
PRIMARY ENDPOINT1
RANKED SECONDARY ENDPOINTS3,8
At Week 12:
At Week 24:
SELECT PRESPECIFIED NONRANKED ENDPOINTS2,3,9,10
DATA LIMITATIONS
Prespecified nonranked endpoints were not controlled for multiplicity; therefore, treatment differences could represent chance findings. No conclusions regarding these comparisons can be made.
BASELINE CHARACTERISTICS3
| MEAN (SD) OR N (%) | MTX n=314 | RINVOQ 15 mg QD n=317 |
|---|---|---|
| Female, n (%) | 240 (76) | 241 (76) |
| Age (years), mean (SD) | 53.3 (12.9) | 51.9 (12.6) |
| Duration since RA diagnosis (years), mean (SD) | 2.6 (5.1) | 2.9 (5.4) |
| RF+ and/or ACPA+, n (%) | 255 (81) | 279 (88) |
| MTX exposure, n (%) | 19 (6) | 30 (9.5) |
| csDMARD exposure, n (%) | 79 (25) | 80 (25) |
| Oral glucocorticoid use, n (%) | 163 (52) | 147 (46) |
| - Dose (mg),* mean (SD) | 6.4 (2.4) | 6.4 (3.1) |
| TJC68, mean (SD) | 26.4 (16.2) | 25.4 (14.4) |
| SJC66, mean (SD) | 16.9 (10.6) | 16.9 (10.4) |
| PtGA (0–100 mm VAS), mean (SD) | 65.8 (21.5) | 66.6 (22.0) |
| PhGA (0–100 mm VAS), mean (SD) | 68.7 (16.5) | 67.1 (17.0) |
| Pain (0–100 mm VAS), mean (SD) | 65.7 (21.5) | 68.4 (20.6) |
| hsCRP (mg/L), mean (SD) | 21.2 (22.1) | 23.0 (27.4) |
| DAS28-CRP, mean (SD) | 5.9 (1.0) | 5.9 (1.0) |
| HAQ-DI, mean (SD) | 1.6 (0.7) | 1.6 (0.7) |
| CDAI, mean (SD) | 40.5 (13.3) | 40.4 (13.3) |
| SDAI, mean (SD) | 42.6 (14.0) | 42.7 (13.9) |
| mTSS, mean (SD) | 13.3 (30.6) | 18.1 (38.2) |
| - Erosion Score, mean (SD) | 6.1 (15.5) | 8.6 (19.3) |
| - Joint Space Narrowing Score, mean (SD) | 7.2 (16.2) | 9.6 (20.1) |
*Prednisone equivalent dose in patients receiving oral glucocorticoids at baseline.
ACPA=anti-citrullinated protein antibody; ACR=American College of Rheumatology; ACR20=improvement of at least 20% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR50=improvement of at least 50% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR70=improvement of at least 70% in tender joint count, swollen joint count, and at least 3 other core criteria; CDAI=Clinical Disease Activity Index; CR=clinical remission; CRP=C-reactive protein; csDMARD=conventional synthetic disease-modifying antirheumatic drug; DAS28-CRP=28-joint disease activity score using C-reactive protein; HAQ-DI=Health Assessment Questionnaire Disability Index; hsCRP=high-sensitivity C-reactive protein; IR=intolerance or inadequate response; JE=joint erosion; JSN=joint space narrowing; LDA=low disease activity; mTSS=modified total Sharp score; MTX=methotrexate; NSAID=nonsteroidal anti-inflammatory drug; PhGA=Physician's Global Assessment; PtGA=patient global assessment; QD=once daily; RA=rheumatoid arthritis; RF=rheumatoid factor; SD=standard deviation; SDAI=Simplified Disease Activity Index; SF-36 (PCS)=36-item short form health survey physical component summary; SJC66=swollen joint count of 66 joints; TJC68=tender joint count of 68 joints; TNFi=tumor necrosis factor inhibitor; UPA=upadacitinib; VAS=visual analog scale.
REFERENCES:
SELECT-NEXT
Adults with moderately to severely active RA who had an inadequate response to csDMARD(s)1
RINVOQ is indicated for TNFi-IR patients1
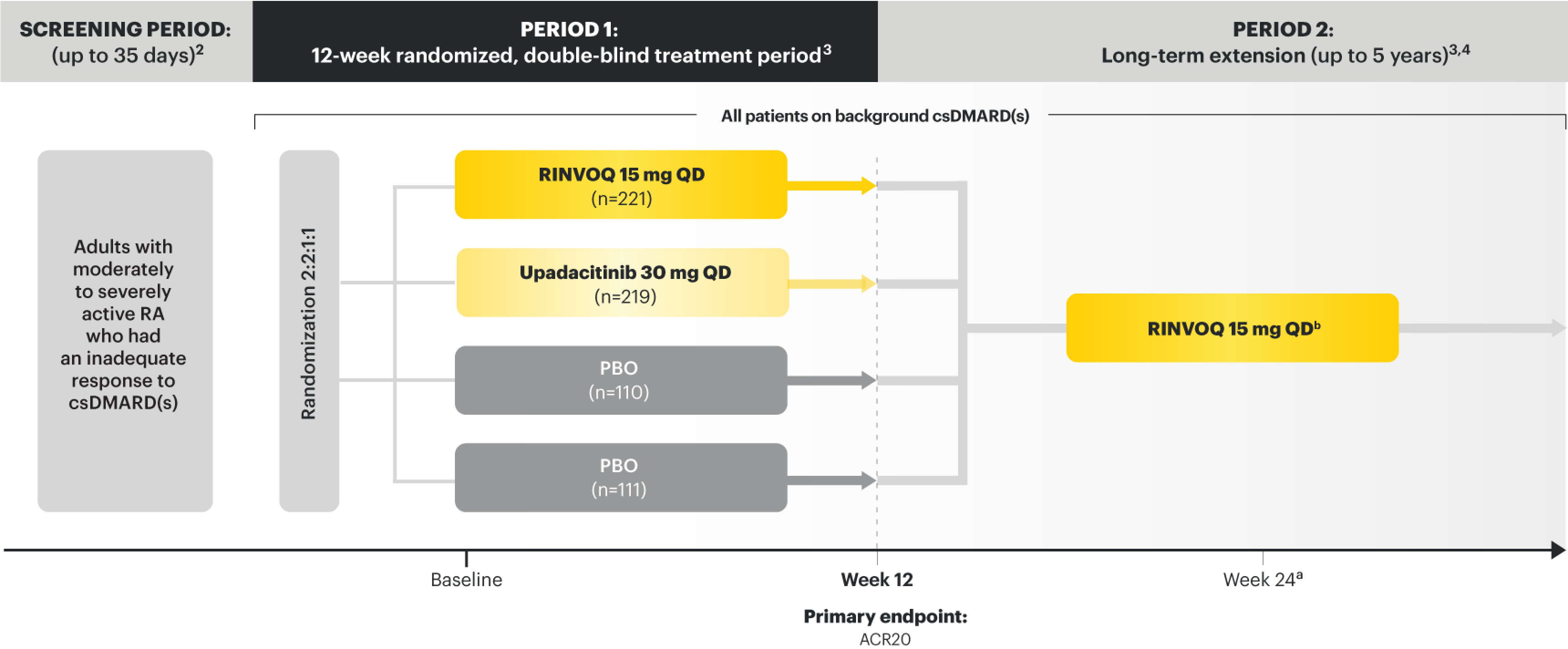
Upadacitinib 30 mg is not an approved dose.
aStarting at Week 24, patients who did not achieve CDAI ≤10 could have initiated or adjusted corticosteroids, NSAIDs, acetaminophen, or ≤2 csDMARDs. Patients who failed to show ≥20% improvement in TJC and SJC compared to baseline at 2 consecutive visits were removed from the study.4
bFollowing a protocol amendment, all patients in the long-term extension received UPA 15 mg QD, including those previously on UPA 30 mg.7
PRIMARY ENDPOINT1
RANKED SECONDARY ENDPOINTS5,6
At Week 12:
SELECT PRESPECIFIED NONRANKED ENDPOINTS6
DATA LIMITATIONS
Prespecified nonranked endpoints were not controlled for multiplicity; therefore, treatment differences could represent chance findings. No conclusions regarding these comparisons can be made.
BASELINE CHARACTERISTICS3
| MEAN (SD) OR N (%) | PBO + csDMARDs n=221 | RINVOQ 15 mg QD + csDMARDs n=221 |
|---|---|---|
| Female, n (%) | 166 (75) | 182 (82) |
| Age (years), mean (SD) | 56.0 (12.2) | 55.3 (11.5) |
| Duration since RA diagnosis (years), mean (SD) | 7.2 (7.5) | 7.3 (7.9) |
| RF+ and/or ACPA+, n (%) | 181 (82) | 184 (83) |
| csDMARD use at baseline | ||
| - MTX alone, n (%) | 141 (64) | 122 (55) |
| - MTX plus other csDMARD, n (%) | 49 (22) | 47 (21) |
| - csDMARD other than MTX, n (%) | 30 (14) | 51 (23) |
| - Missing, n (%) | 1 (<1) | 1 (<1) |
| Prior bDMARD exposure, n (%) | 29 (13) | 27 (12) |
| Oral glucocorticoid use, n (%) | 106 (48) | 96 (43) |
| - Oral glucocorticoid dose* (mg), mean (SD) | 6.3 (2.6) | 6.0 (2.4) |
| TJC68, mean (SD) | 24.7 (15.0) | 25.2 (13.8) |
| SJC66, mean (SD) | 15.4 (9.2) | 16.0 (10.0) |
| PtGA (0–100 mm VAS), mean (SD) | 60.3 (20.5) | 63.1 (21.9) |
| PhGA (0–100 mm VAS), mean (SD) | 64.4 (17.7) | 64.3 (16.2) |
| Pain (0–100 mm VAS), mean (SD) | 61.5 (20.8) | 64.1 (19.5) |
| hsCRP (mg/L), mean (SD) | 12.6 (14.0) | 16.6 (19.2) |
| DAS28-CRP, mean (SD) | 5.6 (0.8) | 5.7 (1.0) |
| HAQ-DI, mean (SD) | 1.4 (0.6) | 1.5 (0.6) |
| CDAI, mean (SD) | 37.8 (11.8) | 38.3 (11.9) |
| SDAI, mean (SD) | 39.0 (11.9) | 39.9 (12.5) |
*Based on prednisone equivalent.
ACPA=anti-citrullinated protein antibody; ACR=American College of Rheumatology; ACR20=improvement of at least 20% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR50=improvement of at least 50% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR70=improvement of at least 70% in tender joint count, swollen joint count, and at least 3 other core criteria; bDMARD=biologic disease-modifying antirheumatic drug; CDAI=Clinical Disease Activity Index; CR=clinical remission; CRP=C-reactive protein; csDMARD=conventional synthetic disease-modifying antirheumatic drug; DAS28-CRP=28-joint disease activity score using C-reactive protein; HAQ-DI=Health Assessment Questionnaire Disability Index; hsCRP=high-sensitivity C-reactive protein; IR=intolerance or inadequate response; JE=joint erosion; JSN=joint space narrowing; LDA=low disease activity; MTX=methotrexate; NSAID=nonsteroidal anti-inflammatory drug; PBO=placebo; PhGA=Physician's Global Assessment; PtGA=patient global assessment; QD=once daily; RA=rheumatoid arthritis; RF=rheumatoid factor; SD=standard deviation; SDAI=Simplified Disease Activity Index; SJC66=swollen joint count of 66 joints; TJC68=tender joint count of 68 joints; TNFi=tumor necrosis factor inhibitor; UPA=upadacitinib; VAS=visual analog scale.
REFERENCES:
US-RNQR-260103
SELECT-BEYOND
Adults with moderately to severely active RA who had an inadequate response or intolerance to bDMARDs1
RINVOQ is indicated for TNFi-IR patients1
Upadacitinib 30 mg is not an approved dose.
aStarting at Week 24, initiation of or change in corticosteroids, NSAIDs, acetaminophen, and csDMARDs was permitted. Patients not achieving response criteria ≥20% improvement in SJC and TJC at 2 consecutive visits were removed from the study.4,5
bFollowing a protocol amendment, all patients in the long-term extension received UPA 15 mg QD, including those previously on UPA 30 mg.8
PRIMARY ENDPOINT1
RANKED SECONDARY ENDPOINTS6,7
At Week 12:
SELECT PRESPECIFIED NONRANKED ENDPOINTS7
DATA LIMITATIONS
Prespecified nonranked endpoints were not controlled for multiplicity; therefore, treatment differences could represent chance findings. No conclusions regarding these comparisons can be made.
BASELINE CHARACTERISTICS6
| MEAN (SD) OR N (%) | PBO + csDMARDs n=169 | RINVOQ 15 mg + csDMARDs n=164 |
|---|---|---|
| Female, n (%) | 143 (85) | 137 (84) |
| Age (years), mean (SD) | 57.6 (11.4) | 56.3 (11.3) |
| Duration since RA diagnosis (years), mean (SD) | 14.5 (9.2) | 12.4 (9.4) |
| RF+ and/or ACPA+, n (%) | 128 (76) | 131 (80) |
| csDMARD use at baseline* | ||
| - MTX alone,† n (%) | 122 (73) | 118 (73) |
| - MTX plus other csDMARD,‡ n (%) | 17 (10) | 19 (12) |
| - MTX dose§ (mg), mean (SD) | 16.6 (4.7) | 17.3 (4.6) |
| - csDMARD other than MTX, n (%) | 29 (17) | 24 (15) |
| - Missing, n | 1 | 3 |
| Prior bDMARD exposure | ||
| - 1, n (%) | 83 (49) | 86 (52) |
| - 2, n (%) | 46 (27) | 40 (24) |
| - ≥3, n (%) | 40 (24) | 38 (23) |
| Inadequate response or intolerance to ≥1 anti-TNF drug | 152 (90) | 146 (89) |
| - Lack of efficacy with ≥1 bDMARD | 159 (94) | 146 (89) |
| - Lack of efficacy with ≥1 anti–IL-6 | 30 (18) | 27 (16) |
| Oral glucocorticoid use, n (%) | 74 (44) | 83 (51) |
| - Oral glucocorticoid dosell (mg), mean (SD) | 6.3 (2.4) | 5.7 (2.4) |
| TJC68, mean (SD) | 28.5 (15.3) | 27.8 (16.3) |
| SJC66, mean (SD) | 16.3 (9.6) | 17.0 (10.8) |
| PtGA (0–100 mm VAS), mean (SD) | 66.3 (22.7) | 67.2 (19.6) |
| PhGA (0–100 mm VAS), mean (SD) | 66.9 (16.9) | 68.7 (16.6) |
| Pain (0–100 mm VAS), mean (SD) | 68.9 (21.0) | 68.2 (19.8) |
| hsCRP (mg/L), mean (SD) | 16.3 (21.1) | 16.2 (18.6) |
| DAS28-CRP, mean (SD) | 5.8 (1.0) | 5.9 (1.0) |
| HAQ-DI, mean (SD) | 1.6 (0.6) | 1.7 (0.6) |
| CDAI, mean (SD) | 41.0 (13.3) | 41.7 (13.3) |
| SDAI, mean (SD) | 42.6 (13.9) | 43.3 (13.8) |
*Oral or parenteral methotrexate (7.5–25 mg per week).
†Data available for 168 patients receiving placebo and 161 patients receiving RINVOQ 15 mg.
‡All combinations allowed except MTX and leflunomide.
§Mean MTX dose calculated only for patients receiving MTX.
‖Based on prednisone equivalent.
ACPA=anti‑citrullinated protein antibodies; ACR20=improvement of at least 20% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR50=improvement of at least 50% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR70=improvement of at least 70% in tender joint count, swollen joint count, and at least 3 other core criteria; bDMARD=biologic disease‑modifying antirheumatic drug; CDAI=Clinical Disease Activity Index; CR=clinical remission; CRP=C‑reactive protein; csDMARD=conventional synthetic disease‑modifying antirheumatic drug; DAS28-CRP=28-joint disease activity score using C-reactive protein; DAS28-ESR=28-joint disease activity score using erythrocyte sedimentation rate; ESR=erythrocyte sedimentation rate; HAQ‑DI=Health Assessment Questionnaire Disability Index; hsCRP=high‑sensitivity C‑reactive protein; IL-6=interleukin 6; IR=intolerance or inadequate response; LDA=low disease activity; MTX=methotrexate; NSAID=nonsteroidal anti‑inflammatory drug; PBO=placebo; PhGA=Physician’s Global Assessment; PtGA=patient global assessment; QD=once daily; RA=rheumatoid arthritis; RF=rheumatoid factor; SD=standard deviation; SDAI=Simplified Disease Activity Index; SF‑36 (PCS)=36‑item short form health survey physical component summary; SJC66=swollen joint count of 66 joints; TJC68=tender joint count of 68 joints; TNFi=tumor necrosis factor inhibitor; UPA=upadacitinib; VAS=visual analog scale.
REFERENCES:
SELECT-COMPARE
Adults with moderately to severely active RA who had an inadequate response to MTX1
RINVOQ is indicated for TNFi-IR patients1
aX-ray imaging was performed at these time points; Week 14 for nonresponder patients, who were rescued.2,3
bRescue criteria: At Weeks 14, 18, and 22, if <20% improvement in TJC and SJC vs baseline; at Week 26, all remaining PBO patients were switched to RINVOQ, and patients receiving RINVOQ or active comparator were switched to active comparator or RINVOQ, respectively, if CDAI >10.2
cStarting at Week 26, initiation or change in background RA medication(s), including corticosteroids, NSAIDs, or acetaminophen was permitted.4
dStarting at Week 48, patients who failed to show ≥20% improvement in TJC and SJC compared to baseline at 2 consecutive visits were removed from the study.5
eAt Week 48, initiation or change in csDMARDs was allowed; however, not all patients received background MTX.5
fPatients continued treatment with UPA or active comparator in a blinded manner until the last patient completed the Week 48 visit and received open-label treatment thereafter.8
PRIMARY ENDPOINT1
SELECT RANKED SECONDARY ENDPOINTS2
At Week 12 vs placebo + MTX:
At Week 12 vs active comparator + MTX:
At Week 26 vs placebo + MTX:
SELECT PRESPECIFIED NONRANKED ENDPOINTS3,9,10
DATA LIMITATIONS
Prespecified nonranked endpoints were not controlled for multiplicity; therefore, treatment differences could represent chance findings. No conclusions regarding these comparisons can be made.
SELECT-COMPARE was not designed to evaluate the efficacy of active comparator + MTX vs placebo + MTX. No conclusions regarding this comparison can be made.
BASELINE CHARACTERISTICS3
| MEAN (SD) OR N (%) | PBO + MTX n=651 | RINVOQ 15 mg QD + MTX n=651 |
|---|---|---|
| Female, n (%) | 512 (79) | 521 (80) |
| Age (years), mean (SD) | 54 (12) | 54 (12) |
| Duration since RA diagnosis (years), mean (SD) | 8 (8) | 8 (8) |
| RF+ and/or anti-CCP+, n (%) | 571 (88) | 566 (87) |
| MTX dose (mg/week), mean (SD) | 16.8 (3.8) | 17.0 (4.2) |
| Prior bDMARD use, n (%) | 63 (10) | 54 (8) |
| Oral glucocorticoid use, n (%) | 392 (60) | 388 (60) |
| - Dose (mg),* mean (SD) | 6.3 (2.4) | 6.2 (2.3) |
| TJC68, mean (SD) | 26 (14) | 26 (15) |
| SJC66, mean (SD) | 16 (9) | 17 (10) |
| PtGA (0–100 mm VAS), mean (SD) | 64 (21) | 64 (22) |
| PhGA (0–100 mm VAS), mean (SD) | 66 (18) | 66 (17) |
| Pain (0–100 mm VAS), mean (SD) | 65 (21) | 66 (21) |
| hsCRP (mg/L), mean (SD) | 18 (22) | 18 (22) |
| DAS28-CRP, mean (SD) | 5.8 (0.9) | 5.8 (1.0) |
| HAQ-DI, mean (SD) | 1.6 (0.6) | 1.6 (0.6) |
| CDAI, mean (SD) | 40 (13) | 40 (13) |
| SDAI, mean (SD) | 41.8 (13.3) | 41.5 (13.6) |
| mTSS, mean (SD) | 36 (52) | 34 (50) |
| - JE score, mean (SD) | 17 (27) | 17 (26) |
| - JSN score, mean (SD) | 19 (26) | 18 (25) |
*Based on prednisone equivalent.
ACPA=anti-citrullinated protein antibody; ACR=American College of Rheumatology; ACR20=improvement of at least 20% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR50=improvement of at least 50% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR70=improvement of at least 70% in tender joint count, swollen joint count, and at least 3 other core criteria; bDMARD=biologic disease‑modifying antirheumatic drug; CCP=cyclic citrullinated peptide; CDAI=Clinical Disease Activity Index; CR=clinical remission; CRP=C‑reactive protein; csDMARD=conventional synthetic disease-modifying antirheumatic drug; DAS28-CRP=28-joint disease activity score using C-reactive protein; DAS28-ESR=28-joint disease activity score using erythrocyte sedimentation rate; EOW=every other week; ESR=erythrocyte sedimentation rate; HAQ‑DI=Health Assessment Questionnaire Disability Index; hsCRP=high-sensitivity C‑reactive protein; IR=intolerance or inadequate response; JE=joint erosion; JSN=joint space narrowing; LDA=low disease activity; mTSS=modified total Sharp score; MTX=methotrexate; NSAID=nonsteroidal anti-inflammatory drug; PBO=placebo; PhGA=Physician's Global Assessment; PtGA=patient global assessment; QD=once per day; RA=rheumatoid arthritis; RF=rheumatoid factor; SD=standard deviation; SDAI=Simplified Disease Activity Index; SF‑36 (PCS)=36-item short form health survey physical component summary; SJC66=swollen joint count of 66 joints; TJC68=tender joint count of 68 joints; TNFi=tumor necrosis factor inhibitor; UPA=upadacitinib; VAS=visual analog scale.
REFERENCES:
SELECT-MONOTHERAPY
Adults with moderately to severely active RA who had an inadequate response to MTX1
RINVOQ is indicated for TNFi-IR patients1
Upadacitinib 30 mg is not an approved dose.
aPatients on cMTX were randomized to receive either RINVOQ 15 mg or upadacitinib 30 mg at Week 14.3
bStarting at Week 26, patients who did not achieve CDAI ≤10 could have initiated or adjusted corticosteroids, NSAIDs, acetaminophen, or ≤2 csDMARDs. Patients who failed to show ≥20% improvement in TJC and SJC compared to baseline at 2 consecutive visits were removed from the study.5
cFollowing a protocol amendment, all patients in the long-term extension received UPA 15 mg QD, including those previously on UPA 30 mg.4
PRIMARY ENDPOINT1
RANKED SECONDARY ENDPOINTS3,6
At Week 14:
SELECT PRESPECIFIED NONRANKED ENDPOINTS3,6
DATA LIMITATIONS
Prespecified nonranked endpoints were not controlled for multiplicity; therefore, treatment differences could represent chance findings. No conclusions regarding these comparisons can be made.
BASELINE CHARACTERISTICS3
| MEAN (SD) OR N (%) | cMTX n=216 | RINVOQ 15 mg QD n=217 |
|---|---|---|
| Female, n (%) | 179 (83) | 174 (80) |
| Age (years), mean (SD) | 55.3 (11.1) | 54.5 (12.2) |
| Duration since RA diagnosis (years), mean (SD) | 5.8 (6.6) | 7.5 (8.9) |
| RF+ and/or ACPA+, n (%) | 169 (78) | 172 (79) |
| Prior MTX dose* (mg/week), mean (SD) | 16.7 (4.4) | 16.8 (4.2) |
| Prior MTX duration (years), mean (SD) | 3.3 (3.9) | 3.8 (4.8) |
| Oral glucocorticoid use, n (%) | 115 (53) | 114 (53) |
| - Oral glucocorticoid dose† (mg), mean (SD) | 6.2 (2.6) | 6.1 (2.5) |
| TJC68, mean (SD) | 25.2 (16.0) | 24.5 (15.1) |
| SJC66, mean (SD) | 16.9 (11.5) | 16.4 (10.9) |
| PtGA (0–100 mm VAS), mean (SD) | 59.6 (21.8) | 62.2 (22.3) |
| PhGA (0–100 mm VAS), mean (SD) | 62.1 (17.5) | 65.7 (18.5) |
| Pain (0–100 mm VAS), mean (SD) | 62.5 (21.3) | 62.3 (22.5) |
| hsCRP (mg/L), mean (SD) | 14.5 (17.3) | 14.0 (16.5) |
| DAS28-CRP, mean (SD) | 5.6 (1.0) | 5.6 (0.9) |
| HAQ-DI, mean (SD) | 1.5 (0.7) | 1.5 (0.7) |
| CDAI, mean (SD) | 37.8 (14.4) | 38.0 (13.1) |
| SDAI, mean (SD) | 39.2 (14.6) | 39.4 (13.4) |
*Prior to receiving study drug. In the control arm, patients continued prior MTX dose as blinded study drug.3
†Prednisone equivalent.
ACPA=anti‑citrullinated protein antibody; ACR=American College of Rheumatology; ACR20=improvement of at least 20% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR50=improvement of at least 50% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR70=improvement of at least 70% in tender joint count, swollen joint count, and at least 3 other core criteria; CDAI=Clinical Disease Activity Index; cMTX=continuous methotrexate; csDMARD=conventional synthetic disease‑modifying antirheumatic drug; CR=clinical remission; CRP=C‑reactive protein; DAS28-CRP=28-joint disease activity score using C-reactive protein; DAS28-ESR=28-joint disease activity score using erythrocyte sedimentation rate; ESR=erythrocyte sedimentation rate; HAQ‑DI=Health Assessment Questionnaire Disability Index; hsCRP=high-sensitivity C‑reactive protein; IR=intolerance or inadequate response; LDA=low disease activity; MTX=methotrexate; NSAID=nonsteroidal anti‑inflammatory drug; PhGA=Physician’s Global Assessment; PtGA=patient global assessment; QD=once daily; RA=rheumatoid arthritis; RF=rheumatoid factor; SD=standard deviation; SDAI=Simplified Disease Activity Index; SF‑36 (PCS)=36-item short form health survey physical component summary; SJC66=swollen joint count of 66 joints; TJC68=tender joint count of 68 joints; TNFi=tumor necrosis factor inhibitor; UPA=upadacitinib; VAS=visual analog scale.
REFERENCES:
SELECT-SWITCH
Head-to-head study powered to evaluate superiority of RINVOQ vs HUMIRA (adalimumab) in RA patients who had inadequate response or intolerance to 1 TNFi2
A 12-week, randomized, double-blind, active-comparator–controlled study of 491 adult patients with moderate to severe RA who did not respond to 1 TNFi (non-adalimumab). Designed to evaluate superiority of continuing TNFi therapy with HUMIRA (adalimumab) vs switching to RINVOQ (upadacitinib).
PRIMARY ENDPOINT2
SELECT RANKED SECONDARY ENDPOINTS2
At Week 12 vs HUMIRA:
SELECT PRESPECIFIED NONRANKED ENDPOINTS2
At all visits:
| MEAN (SD) Unless otherwise stated |
RINVOQ 15 mg QD + MTX (n=245) | HUMIRA 40 mg EOW + MTX n=246* |
|---|---|---|
| Parameter | ||
| Age (years) | 55.3 (12.7) | 55.9 (12.5) |
| Age ≥65 years, n (%) | 57 (23.3) | 72 (29.3) |
| Female, n (%) | 189 (77.1) | 191 (77.6) |
| BMI (kg/m2) | 29.4 (6.5) | 28.8 (7.0) |
| RA duration since diagnosis (years) | 10.1 (8.5) (n=244) | 10.3 (9.3) |
| Disease Characteristics | ||
| DAS28-CRP | 5.7 (0.8) (n=235) | 5.7 (0.8) (n=236) |
| DAS28-ESR | 6.3 (0.9) (n=234) | 6.4 (0.9) (n=235) |
| TJC68 | 22.4 (12.3) | 22.8 (12.6) |
| SJC66 | 15.5 (6.6) | 15.9 (8.3) |
| hsCRP (mg/L) | 16.8 (25.4) (n=245) | 14.0 (17.6) |
| ESR (mm/hr) | 37.1 (23.4) (n=243) | 38.9 (24.4) (n=245) |
| PtGA (0–10 NRS) | 7.1 (1.9) (n=235) | 7.4 (1.9) (n=236) |
| PhGA (0–10 NRS) | 7.0 (1.6) | 6.9 (1.6) |
| Pain (0–10 NRS) | 7.4 (1.9) | 7.4 (1.9) (n=232) |
| HAQ-DI | 1.6 (0.6) (n=234) | 1.6 (0.6) (n=234) |
| FACIT-Fatigue | 26.8 (11.5) (n=234) | 26.8 (10.5) (n=233) |
| Concomitant Therapies | ||
| Patients receiving oral corticosteroid at baseline, n (%) | 99 (40.4) | 100 (40.7) |
| Oral steroid dose (prednisone equivalent) at baseline (mg/day) | 6.4 (2.7) (n=99) | 6.7 (3.2) (n=100) |
| MTX dose at baseline (mg/week), median | 15.0 | 15.0 (n=245) |
| NSAIDs | 128 (52.2) | 111 (45.1) |
| Patient History, n (%) | ||
| HZ vaccination | 35 (14.6) | 31 (12.8) |
| History of VTE | 2 (0.8) | 2 (0.8) |
| History of CV event | 18 (7.3) | 11 (4.5) |
| Number of CV risk factorsa, n (%) | ||
| 0 | 72 (29.4) | 65 (26.4) |
| 1 | 94 (38.4) | 107 (43.5) |
| 2 | 58 (23.7) | 61 (24.8) |
| 3+ | 21 (8.6) | 13 (5.3) |
| CV risk factors at baseline, n (%) | ||
| Hypertension | 90 (36.7) | 85 (34.6) |
| Diabetes mellitus | 6 (2.4) | 2 (0.8) |
| History of tobacco/nicotine use (current/former) | 89 (36.3) | 77 (31.3) |
| Elevated LDL-Cb | 42 (17.1) | 65 (26.4) |
| Low HDL-Cc | 36 (14.7) | 32 (13.0) |
| Reason for discontinuation of prior TNFi, n (%) | ||
| Intolerance | 25 (10.2) | 27 (11.0) |
| Inadequate response | 220 (89.8) | 219 (89.0) |
| Type of inadequate response to prior TNFi, n (%) | ||
| Primary nonresponder | 121 (55.8) | 115 (54.0) |
| Secondary nonresponder | 96 (44.2) | 98 (46.0) |
| Missing | 3 | 6 |
| Prior TNFi administered, n (%) | ||
| Etanercept | 165 (67.3) | 170 (69.1) |
| Certolizumab | 40 (16.3) | 35 (14.2) |
| Golimumab | 24 (9.8) | 21 (8.5) |
| Infliximab | 15 (6.1) | 13 (5.3) |
| Adalimumab† | 0 | 1 (0.4) |
*Patients entered the study while receiving a stable dose of MTX (15–25 mg/week). MTX was not considered an ancillary drug in the study.2
†Protocol deviations.2
aCV risk factors included CV event, hypertension, diabetes mellitus, tobacco/nicotine use, elevated LDL-C, and lowered HDL‑C.
b≥3.36 mmol/L (ie, >129.9 mg/dL).
c<1.034 mmol/L (ie, <18.6 mg/dL).
ACR=American College of Rheumatology; BMI=body mass index; CDAI=Clinical Disease Activity Index; CRP=C-reactive protein; CV=cardiovascular; DAS28-CRP=Disease Activity Score in 28 joints using C-reactive protein; DAS28-ESR=28-joint Disease Activity Score using erythrocyte sedimentation rate; EOW=every other week; ESR=erythrocyte sedimentation rate; FACIT-Fatigue=Functional Assessment of Chronic Illness Therapy-Fatigue; HAQ-DI=Health Assessment Questionnaire-Disability Index; HDL-C=high-density lipoprotein cholesterol; hsCRP=high-sensitivity C-reactive protein; HZ=herpes zoster; IR=intolerance or inadequate response; LDA=low disease activity; LDL-C=low-density lipoprotein cholesterol; MACE=major adverse cardiovascular event; MTX=methotrexate; NSAID=nonsteroidal anti-inflammatory drug; PhGA=Physician's Global Assessment; PtGA=patient global assessment; primary nonresponder=patient who did not respond to prior TNFi treatment; QD=once daily; RA=rheumatoid arthritis; SC=subcutaneous; SD=standard deviation; SDAI=Simplified Disease Activity Index; secondary nonresponder=patient who initially responded to prior TNFi treatment but lost response over time; SJC66=swollen joint count of 66 joints; TJC68=tender joint count of 68 joints; TNFi=tumor necrosis factor inhibitor; VTE=venous thromboembolism.
REFERENCES:
SELECT-EARLY
Adults with moderately to severely active RA who were MTX‑naïve1
RINVOQ is indicated for TNFi-IR patients1
Upadacitinib 30 mg is not an approved dose.
aInitially 947 patients were randomized in the study, but 2 patients were never dosed.
bX-ray images of hands and feet obtained at these time points.2
cStarting at Week 12, patients with ≤20% improvement in TJC and SJC compared to baseline at 2 consecutive visits continued blinded therapy and optimized background RA medications (corticosteroids, NSAIDs, and/or low‑potency analgesics).3,4
dAt Week 26, patients with CDAI ≤2.8 continued their original study drug; background medications (NSAIDs, corticosteroids, and/or low‑potency analgesics, and csDMARDs) were optimized in patients with CDAI >2.8 but ≥20% improvement in TJC and SJC; among patients with CDAI >2.8 and <20% improvement in TJC and SJC, RINVOQ 15 mg or upadacitinib 30 mg were added by re‑randomization according to 1:1 ratio for those initially randomized to MTX, and MTX was added for those initially randomized to RINVOQ 15 mg or upadacitinib 30 mg.2,5
eStarting at Week 48, patients who did not achieve ≥20% improvement in both TJC and SJC at 2 consecutive visits were removed from the study. Initiation of or change in background RA medications (NSAIDs, corticosteroids, low-potency analgesics, and csDMARDs; not all patients received background MTX) is allowed at anytime during Period 2.6
fFollowing a protocol amendment, all patients in the long-term extension who were previously receiving UPA 30 mg received RINVOQ 15 mg.11
PRIMARY ENDPOINT1
RANKED SECONDARY ENDPOINTS3,8
At Week 12:
At Week 24:
SELECT PRESPECIFIED NONRANKED ENDPOINTS2,3,9,10
DATA LIMITATIONS
Prespecified nonranked endpoints were not controlled for multiplicity; therefore, treatment differences could represent chance findings. No conclusions regarding these comparisons can be made.
BASELINE CHARACTERISTICS3
| MEAN (SD) OR N (%) | MTX n=314 | RINVOQ 15 mg QD n=317 |
|---|---|---|
| Female, n (%) | 240 (76) | 241 (76) |
| Age (years), mean (SD) | 53.3 (12.9) | 51.9 (12.6) |
| Duration since RA diagnosis (years), mean (SD) | 2.6 (5.1) | 2.9 (5.4) |
| RF+ and/or ACPA+, n (%) | 255 (81) | 279 (88) |
| MTX exposure, n (%) | 19 (6) | 30 (9.5) |
| csDMARD exposure, n (%) | 79 (25) | 80 (25) |
| Oral glucocorticoid use, n (%) | 163 (52) | 147 (46) |
| - Dose (mg),* mean (SD) | 6.4 (2.4) | 6.4 (3.1) |
| TJC68, mean (SD) | 26.4 (16.2) | 25.4 (14.4) |
| SJC66, mean (SD) | 16.9 (10.6) | 16.9 (10.4) |
| PtGA (0–100 mm VAS), mean (SD) | 65.8 (21.5) | 66.6 (22.0) |
| PhGA (0–100 mm VAS), mean (SD) | 68.7 (16.5) | 67.1 (17.0) |
| Pain (0–100 mm VAS), mean (SD) | 65.7 (21.5) | 68.4 (20.6) |
| hsCRP (mg/L), mean (SD) | 21.2 (22.1) | 23.0 (27.4) |
| DAS28-CRP, mean (SD) | 5.9 (1.0) | 5.9 (1.0) |
| HAQ-DI, mean (SD) | 1.6 (0.7) | 1.6 (0.7) |
| CDAI, mean (SD) | 40.5 (13.3) | 40.4 (13.3) |
| SDAI, mean (SD) | 42.6 (14.0) | 42.7 (13.9) |
| mTSS, mean (SD) | 13.3 (30.6) | 18.1 (38.2) |
| - Erosion Score, mean (SD) | 6.1 (15.5) | 8.6 (19.3) |
| - Joint Space Narrowing Score, mean (SD) | 7.2 (16.2) | 9.6 (20.1) |
*Prednisone equivalent dose in patients receiving oral glucocorticoids at baseline.
ACPA=anti-citrullinated protein antibody; ACR=American College of Rheumatology; ACR20=improvement of at least 20% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR50=improvement of at least 50% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR70=improvement of at least 70% in tender joint count, swollen joint count, and at least 3 other core criteria; CDAI=Clinical Disease Activity Index; CR=clinical remission; CRP=C-reactive protein; csDMARD=conventional synthetic disease-modifying antirheumatic drug; DAS28-CRP=28-joint disease activity score using C-reactive protein; HAQ-DI=Health Assessment Questionnaire Disability Index; hsCRP=high-sensitivity C-reactive protein; IR=intolerance or inadequate response; JE=joint erosion; JSN=joint space narrowing; LDA=low disease activity; mTSS=modified total Sharp score; MTX=methotrexate; NSAID=nonsteroidal anti-inflammatory drug; PhGA=Physician's Global Assessment; PtGA=patient global assessment; QD=once daily; RA=rheumatoid arthritis; RF=rheumatoid factor; SD=standard deviation; SDAI=Simplified Disease Activity Index; SF-36 (PCS)=36-item short form health survey physical component summary; SJC66=swollen joint count of 66 joints; TJC68=tender joint count of 68 joints; TNFi=tumor necrosis factor inhibitor; UPA=upadacitinib; VAS=visual analog scale.
REFERENCES:
SELECT-NEXT
Adults with moderately to severely active RA who had an inadequate response to csDMARD(s)1
RINVOQ is indicated for TNFi-IR patients1
Upadacitinib 30 mg is not an approved dose.
aStarting at Week 24, patients who did not achieve CDAI ≤10 could have initiated or adjusted corticosteroids, NSAIDs, acetaminophen, or ≤2 csDMARDs. Patients who failed to show ≥20% improvement in TJC and SJC compared to baseline at 2 consecutive visits were removed from the study.4
bFollowing a protocol amendment, all patients in the long-term extension received UPA 15 mg QD, including those previously on UPA 30 mg.7
PRIMARY ENDPOINT1
RANKED SECONDARY ENDPOINTS5,6
At Week 12:
SELECT PRESPECIFIED NONRANKED ENDPOINTS6
DATA LIMITATIONS
Prespecified nonranked endpoints were not controlled for multiplicity; therefore, treatment differences could represent chance findings. No conclusions regarding these comparisons can be made.
BASELINE CHARACTERISTICS3
| MEAN (SD) OR N (%) | PBO + csDMARDs n=221 | RINVOQ 15 mg QD + csDMARDs n=221 |
|---|---|---|
| Female, n (%) | 166 (75) | 182 (82) |
| Age (years), mean (SD) | 56.0 (12.2) | 55.3 (11.5) |
| Duration since RA diagnosis (years), mean (SD) | 7.2 (7.5) | 7.3 (7.9) |
| RF+ and/or ACPA+, n (%) | 181 (82) | 184 (83) |
| csDMARD use at baseline | ||
| - MTX alone, n (%) | 141 (64) | 122 (55) |
| - MTX plus other csDMARD, n (%) | 49 (22) | 47 (21) |
| - csDMARD other than MTX, n (%) | 30 (14) | 51 (23) |
| - Missing, n (%) | 1 (<1) | 1 (<1) |
| Prior bDMARD exposure, n (%) | 29 (13) | 27 (12) |
| Oral glucocorticoid use, n (%) | 106 (48) | 96 (43) |
| - Oral glucocorticoid dose* (mg), mean (SD) | 6.3 (2.6) | 6.0 (2.4) |
| TJC68, mean (SD) | 24.7 (15.0) | 25.2 (13.8) |
| SJC66, mean (SD) | 15.4 (9.2) | 16.0 (10.0) |
| PtGA (0–100 mm VAS), mean (SD) | 60.3 (20.5) | 63.1 (21.9) |
| PhGA (0–100 mm VAS), mean (SD) | 64.4 (17.7) | 64.3 (16.2) |
| Pain (0–100 mm VAS), mean (SD) | 61.5 (20.8) | 64.1 (19.5) |
| hsCRP (mg/L), mean (SD) | 12.6 (14.0) | 16.6 (19.2) |
| DAS28-CRP, mean (SD) | 5.6 (0.8) | 5.7 (1.0) |
| HAQ-DI, mean (SD) | 1.4 (0.6) | 1.5 (0.6) |
| CDAI, mean (SD) | 37.8 (11.8) | 38.3 (11.9) |
| SDAI, mean (SD) | 39.0 (11.9) | 39.9 (12.5) |
*Based on prednisone equivalent.
ACPA=anti-citrullinated protein antibody; ACR=American College of Rheumatology; ACR20=improvement of at least 20% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR50=improvement of at least 50% in tender joint count, swollen joint count, and at least 3 other core criteria; ACR70=improvement of at least 70% in tender joint count, swollen joint count, and at least 3 other core criteria; bDMARD=biologic disease-modifying antirheumatic drug; CDAI=Clinical Disease Activity Index; CR=clinical remission; CRP=C-reactive protein; csDMARD=conventional synthetic disease-modifying antirheumatic drug; DAS28-CRP=28-joint disease activity score using C-reactive protein; HAQ-DI=Health Assessment Questionnaire Disability Index; hsCRP=high-sensitivity C-reactive protein; IR=intolerance or inadequate response; JE=joint erosion; JSN=joint space narrowing; LDA=low disease activity; MTX=methotrexate; NSAID=nonsteroidal anti-inflammatory drug; PBO=placebo; PhGA=Physician's Global Assessment; PtGA=patient global assessment; QD=once daily; RA=rheumatoid arthritis; RF=rheumatoid factor; SD=standard deviation; SDAI=Simplified Disease Activity Index; SJC66=swollen joint count of 66 joints; TJC68=tender joint count of 68 joints; TNFi=tumor necrosis factor inhibitor; UPA=upadacitinib; VAS=visual analog scale.
REFERENCES:
US-RNQR-260103
RINVOQ vs
HUMIRA® (adalimumab)
SELECT-SWITCH Study in RA
Explore head-to-head data for RINVOQ vs HUMIRA in moderate to severe rheumatoid arthritis patients who have had an inadequate response or intolerance to 1 TNFi.